

Increased interleukin-6/C-reactive protein levels are associated with the upregulation of the adenosine pathway and serve as potential markers of therapeutic resistance to immune checkpoint inhibitor-based therapies in non-small cell lung cancer
- PMID: 37852738
- PMCID: PMC10603340
- DOI: 10.1136/jitc-2023-007310
Increased interleukin-6/C-reactive protein levels are associated with the upregulation of the adenosine pathway and serve as potential markers of therapeutic resistance to immune checkpoint inhibitor-based therapies in non-small cell lung cancer
Abstract
Background: Systemic immune activation, hallmarked by C-reactive protein (CRP) and interleukin-6 (IL-6), can modulate antitumor immune responses. In this study, we evaluated the role of IL-6 and CRP in the stratification of patients with non-small cell lung cancer (NSCLC) treated with immune checkpoint inhibitors (ICIs). We also interrogated the underlying immunosuppressive mechanisms driven by the IL-6/CRP axis.
Methods: In cohort A (n=308), we estimated the association of baseline CRP with objective response rate (ORR), progression-free survival (PFS), and overall survival (OS) in patients with NSCLC treated with ICIs alone or with chemo-immunotherapy (Chemo-ICI). Baseline tumor bulk RNA sequencing (RNA-seq) of lung adenocarcinomas (LUADs) treated with pembrolizumab (cohort B, n=59) was used to evaluate differential expression of purine metabolism, as well as correlate IL-6 expression with PFS. CODEFACS approach was applied to deconvolve cohort B to characterize the tumor microenvironment by reconstructing the cell-type-specific transcriptome from bulk expression. Using the LUAD cohort from The Cancer Genome Atlas (TCGA) we explored the correlation between IL-6 expression and adenosine gene signatures. In a third cohort (cohort C, n=18), plasma concentrations of CRP, adenosine 2a receptor (A2aR), and IL-6 were measured using ELISA.
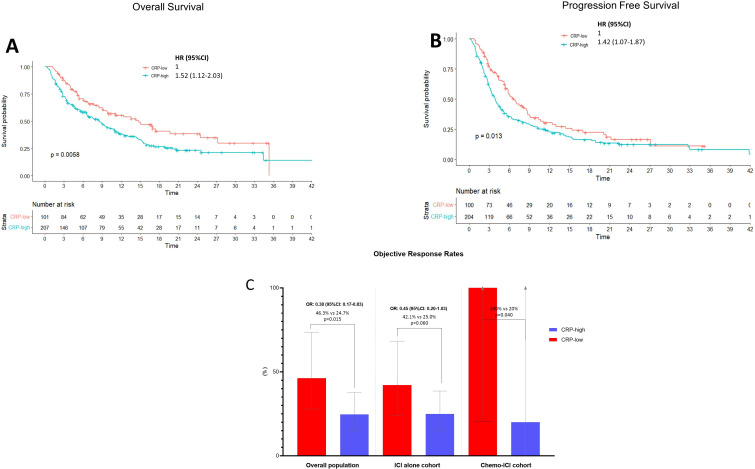
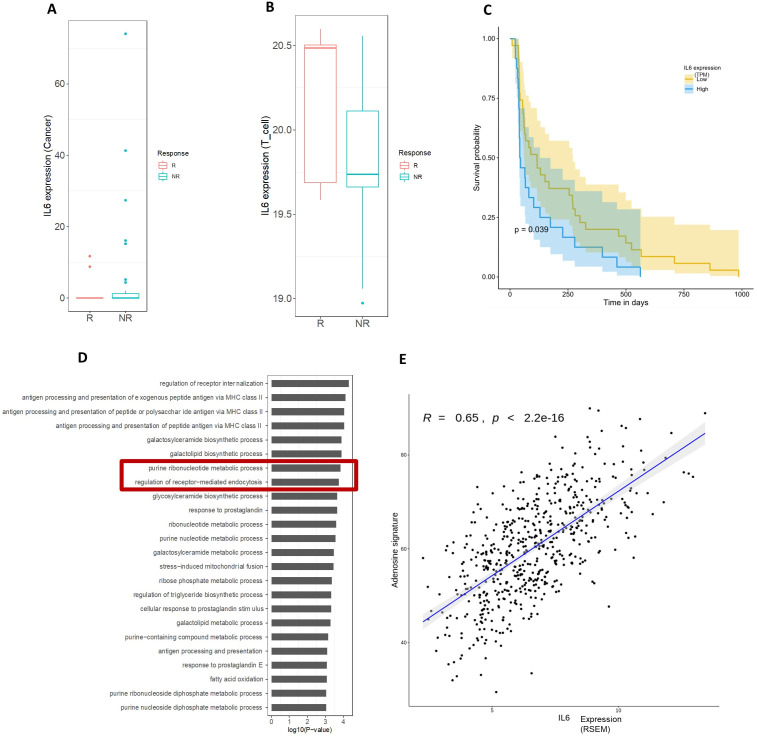
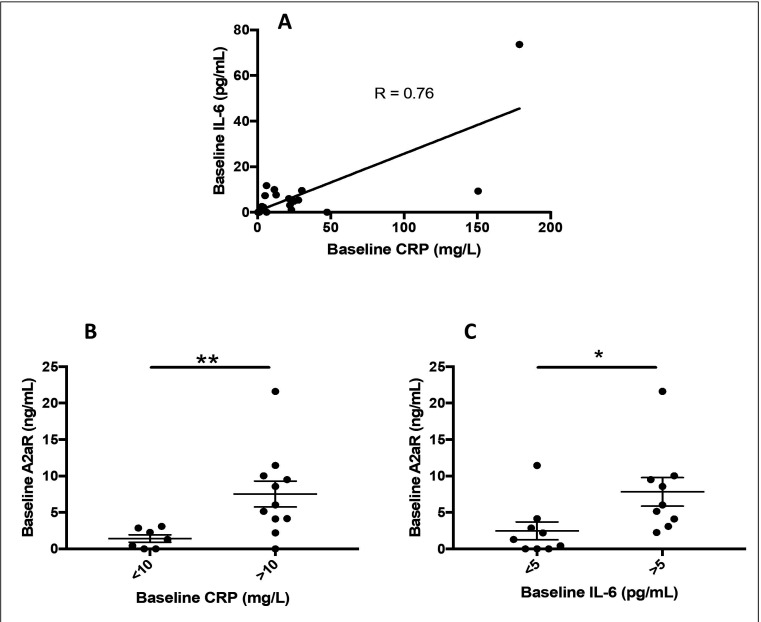
Results: In cohort A, 67.2% of patients had a baseline CRP≥10 mg/L (CRP-H). Patients with CRP-H achieved shorter OS (8.6 vs 14.8 months; p=0.006), shorter PFS (3.3 vs 6.6 months; p=0.013), and lower ORR (24.7% vs 46.3%; p=0.015). After adjusting for relevant clinical variables, CRP-H was confirmed as an independent predictor of increased risk of death (HR 1.51, 95% CI: 1.09 to 2.11) and lower probability of achieving disease response (OR 0.34, 95% CI: 0.13 to 0.89). In cohort B, RNA-seq analysis demonstrated higher IL-6 expression on tumor cells of non-responders, along with a shorter PFS (p<0.05) and enrichment of the purinergic pathway. Within the TCGA LUAD cohort, tumor IL-6 expression strongly correlated with the adenosine signature (R=0.65; p<2.2e-16). Plasma analysis in cohort C demonstrated that CRP-H patients had a greater median baseline level of A2aR (6.0 ng/mL vs 1.3 ng/mL; p=0.01).
Conclusions: This study demonstrates CRP as a readily available blood-based prognostic biomarker in ICI-treated NSCLC. Additionally, we elucidate a potential link of the CRP/IL-6 axis with the immunosuppressive adenosine signature pathway that could drive inferior outcomes to ICIs in NSCLC and also offer novel therapeutic avenues.
Keywords: Adenosine; Immune Checkpoint Inhibitors; Inflammation; Lung Neoplasms; Tumor Microenvironment.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: The authors disclose no conflicts of interest in relation to the published work. AC received grants for consultancies/advisory boards: BMS, MSD, OncoC4, IQVIA, Roche, GSK, AstraZeneca, Access Infinity, Ardelis Health. He also received speaker fees from AstraZeneca, EISAI, MSD and Pierre-Fabre. DJP received lecture fees from ViiV Healthcare, Bayer Healthcare, AstraZeneca, Roche, IPSEN and travel expenses from BMS and Bayer Healthcare; consulting fees for Mina Therapeutics, EISAI, Roche, AstraZeneca, DaVolterra, Exact Sciences, MURSLA, Avamune, BMS; received research funding (to institution) from MSD, BMS, GSK.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous