

The effect of conditioning regimen and prescribed medications on hyposalivation in haematopoietic cell transplantation (HCT) patients: an 18-month prospective longitudinal study
- PMID: 37853264
- PMCID: PMC10713764
- DOI: 10.1007/s00784-023-05327-1
The effect of conditioning regimen and prescribed medications on hyposalivation in haematopoietic cell transplantation (HCT) patients: an 18-month prospective longitudinal study
Abstract
Objectives: Haematopoietic cell transplantation (HCT) preceded by a conditioning regimen is an established treatment option for (non)malignant haematologic disorders. We aim to describe the development of hyposalivation over time in HCT recipients, and determine risk indicators.
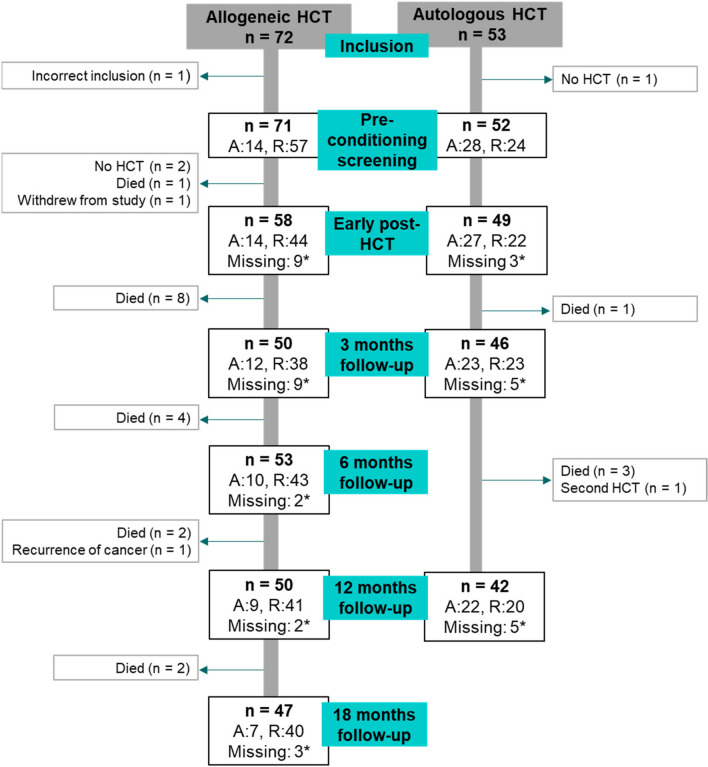
Materials and methods: A multi-centre prospective longitudinal observational study was conducted. Unstimulated (UWS) and stimulated (SWS) whole saliva was collected before HCT, early post-HCT, and after 3, 6, 12, and 18 months. The effect of type of transplantation (allogeneic vs autologous) and intensity (full vs reduced) of the conditioning regimen on hyposalivation (UWS < 0.2 mL/min; SWS < 0.7 mL/min) was explored.
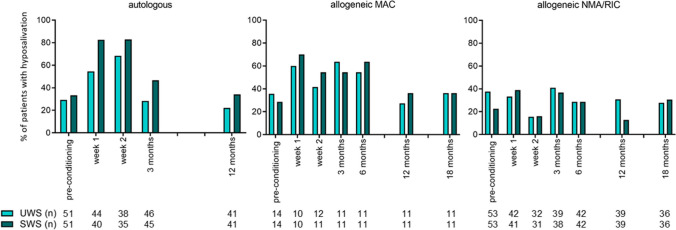
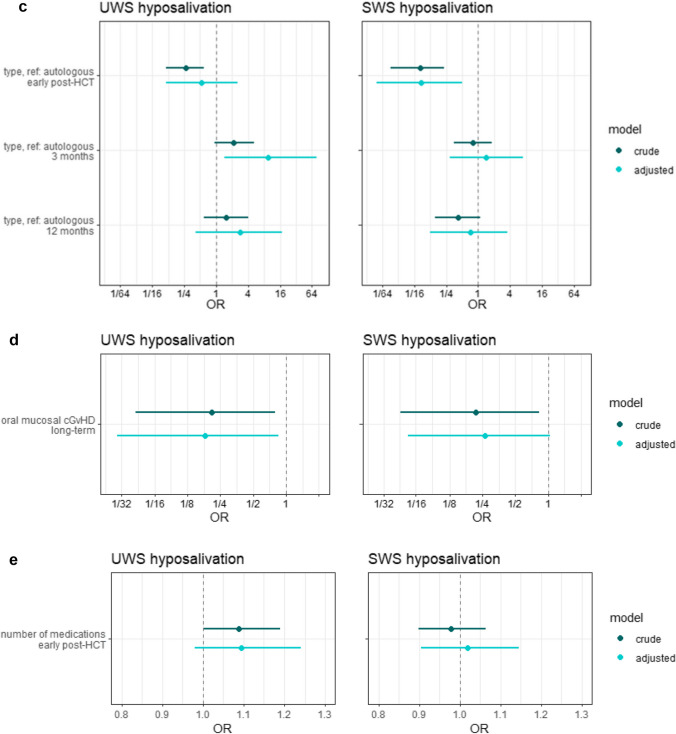
Results: A total of 125 HCT recipients were included. More than half of the patients had hyposalivation early post-HCT; a quarter still had hyposalivation after 12 months. The conditioning intensity was a risk indicator in the development of hyposalivation of both UWS (OR: 3.9, 95% CI: 1.6-10.6) and SWS (OR: 8.2, 95% CI: 2.9-24.6). After 3 and 12 months, this effect was not statistically significant anymore.
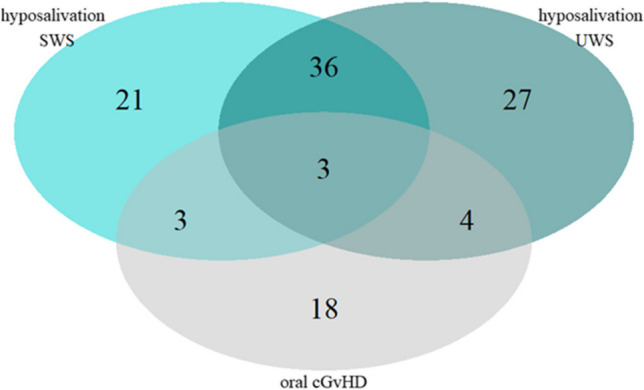
Conclusions: Hyposalivation affects the majority of patients early post-HCT. The conditioning intensity and the type of transplantation were significant risk indicators in the development of hyposalivation. The number of prescribed medications, total body irradiation as part of the conditioning regimen and oral mucosal graft-versus-host disease did not influence hyposalivation significantly.
Clinical relevance: Because of the high prevalence of hyposalivation, HCT recipients will have an increased risk of oral complications. It might be reasonable to plan additional check-ups in the dental practice and consider additional preventive strategies.
Keywords: Haematopoietic cell transplantation; Hyposalivation; Medications; Salivary flow rate.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Niederwieser D, Baldomero H, Szer J, Gratwohl M, Aljurf M, Atsuta Y, Bouzas LF, Confer D, Greinix H, Horowitz M, Iida M, Lipton J, Mohty M, Novitzky N, Nunez J, Passweg J, Pasquini MC, Kodera Y, Apperley J, Seber A, Gratwohl A. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the Worldwide Network for Blood and Marrow Transplantation Group including the global survey. Bone Marrow Transplant. 2016;51(6):778–785. doi: 10.1038/bmt.2016.18. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
