

Risk factors for renal outcomes in children with antineutrophil cytoplasmic antibody-associated vasculitis: a nationwide retrospective study in China
- PMID: 37853276
- PMCID: PMC11136751
- DOI: 10.1007/s12519-023-00753-3
Risk factors for renal outcomes in children with antineutrophil cytoplasmic antibody-associated vasculitis: a nationwide retrospective study in China
Abstract
Background: Pediatric antineutrophil cytoplasmic antibody-associated vasculitis (AAV) is a life-threatening systemic vasculitis featured by liability to renal involvement. However, there are few studies on the risk factors and predictive models for renal outcomes of AAV in children.
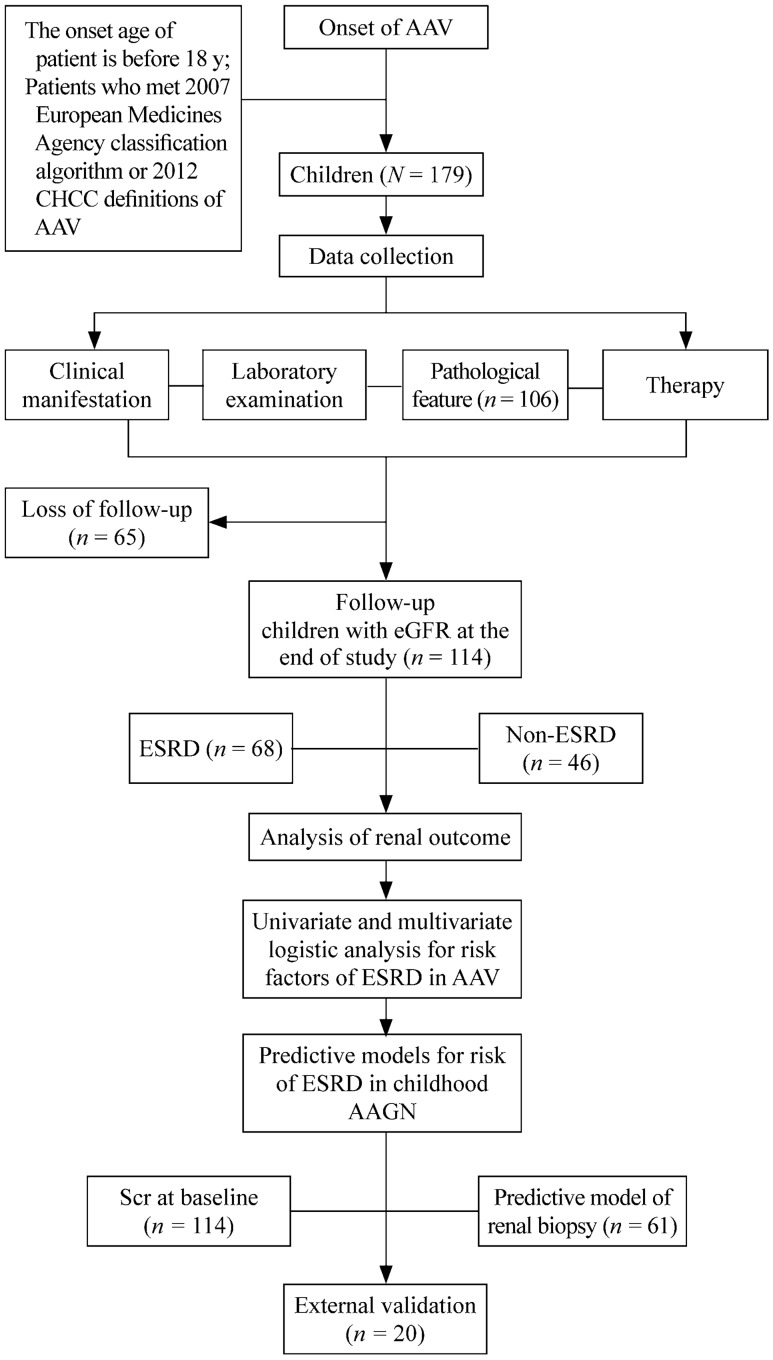
Methods: Data from 179 AAV children in multiple centers between January 2012 and March 2020 were collected retrospectively. The risk factors and predictive model of end-stage renal disease (ESRD) in AAV were explored.
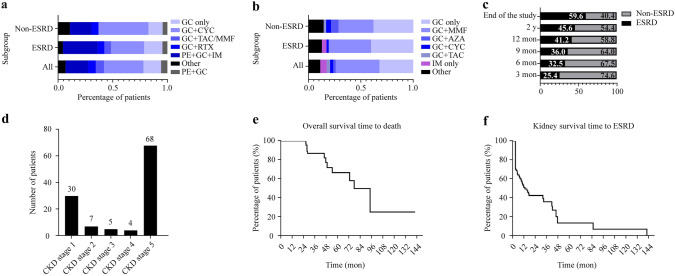
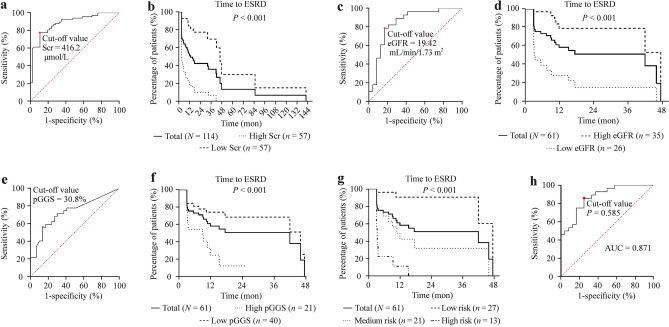
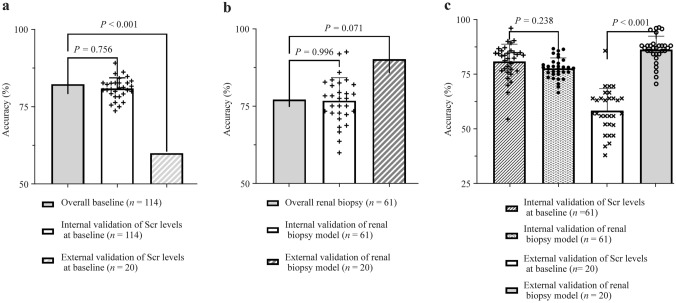
Results: Renal involvement was the most typical manifestation (95.5%), and the crescent was the predominant pathological lesion (84.9%). The estimated glomerular filtration rate (eGFR) was evaluated in 114 patients, of whom 59.6% developed ESRD, and the median time to ESRD was 3.20 months. The eGFR [P = 0.006, odds ratio (OR) = 0.955, 95% confidence interval (CI) = 0.924-0.987] and the percentages of global glomerulosclerosis (pGGS; P = 0.018, OR = 1.060, 95% CI = 1.010-1.112) were independent risk factors for ESRD of renal biopsy. Based on the pGGS and eGFR at renal biopsy, we developed three risk grades of ESRD and one predictive model. The Kaplan‒Meier curve indicated that renal outcomes were significantly different in different risk grades (P < 0.001). Compared with serum creatinine at baseline, the predictive model had higher accuracy (0.86 versus 0.58, P < 0.001) and a lower coefficient of variation (0.07 versus 0.92) in external validation.
Conclusions: Renal involvement is the most common manifestation of pediatric AAV in China, of which more than half deteriorates into ESRD. The predictive model based on eGFR at renal biopsy and the pGGS may be stable and accurate in speculating the risk of ESRD in AAV children. Supplementary file 2 (MP4 18937 KB).
Keywords: Antineutrophil cytoplasmic antibody; End-stage renal disease; Glomerulonephritis; Pediatric nephrology; Vasculitis.
© 2023. The Author(s).
Conflict of interest statement
Authors Jian-Hua Mao, Hong Xu, and Ai-Hua Zhang are members of the Editorial Board for
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
