

Intravascular Hemolysis and AKI in Children Undergoing Extracorporeal Membrane Oxygenation
- PMID: 37853572
- PMCID: PMC10695640
- DOI: 10.34067/KID.0000000000000253
Intravascular Hemolysis and AKI in Children Undergoing Extracorporeal Membrane Oxygenation
Abstract
Key Points:
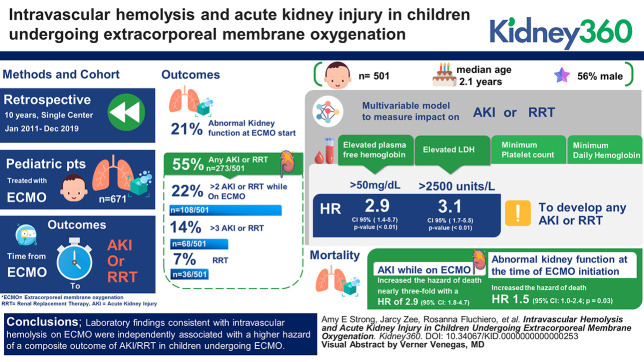
The incidence of AKI while undergoing ECMO in pediatric patients is high and independently increases mortality.
Laboratory markers consistent with intravascular hemolysis increase the hazard of a composite outcome of AKI or RRT while undergoing ECMO.
Further research into appropriate monitoring or treatment of ECMO-associated hemolysis may lead to important interventions to prevent AKI.
Background: AKI is common in patients requiring extracorporeal membrane oxygenation (ECMO), with a variety of proposed mechanisms. We sought to describe the effect of laboratory evidence of ECMO-associated intravascular hemolysis on AKI and RRT.
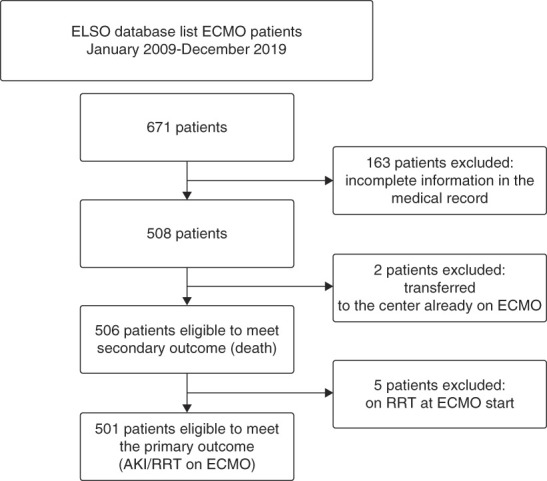
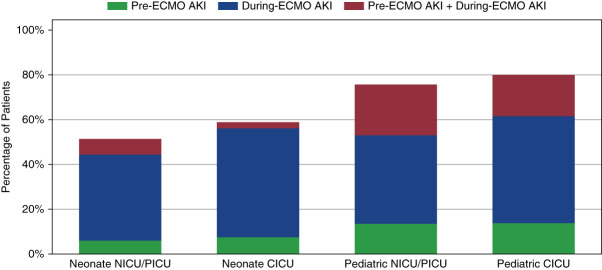
Methods: This retrospective cohort study included patients treated with ECMO at a single center over 10 years. The primary outcome was a composite of time to RRT or AKI (by creatinine-based Kidney Disease Improving Global Outcomes criteria) after ECMO start. Serum creatinine closest to ECMO start time was considered the pre-ECMO baseline and used to determine abnormal kidney function at ECMO start. The patient's subsequent creatinine values were used to identify AKI on ECMO. Multivariable cause-specific Cox proportional hazards models were used to assess the effect of separate markers of intravascular hemolysis on the time to the composite outcome after controlling for confounders.
Results: Five hundred and one children were evaluated with a median age 1.2 years, 56% male. Four separate multivariable models, each with a different marker of hemolysis (plasma-free hemoglobin, lactate dehydrogenase (LDH), minimum platelet count, and minimum daily hemoglobin), were used to examine the effect on the composite outcome of AKI/RRT. An elevated plasma-free hemoglobin, the most specific of these hemolysis markers, demonstrated an almost three-fold higher adjusted hazard for the composite outcome (hazard ratio [HR], 2.9; P value < 0.01; 95% confidence interval [CI], 1.4 to 5.6). Elevated LDH was associated with an adjusted HR of 3.1 (P value < 0.01; 95% CI, 1.7 to 5.5). Effect estimates were also pronounced in a composite outcome of only more severe AKI, stage 2+ AKI/RRT: HR 6.6 (P value < 0.01; 95% CI, 3.3 to 13.2) for plasma-free hemoglobin and 2.8 (P value < 0.01; 95% CI, 1.5 to 5.6) for LDH.
Conclusions: Laboratory findings consistent with intravascular hemolysis on ECMO were independently associated with a higher hazard of a composite outcome of AKI/RRT in children undergoing ECMO.
Conflict of interest statement
M.R. Denburg reports consultancy agreement with TriSalus Life Sciences (spouse); ownership interest in In-Bore LLC (spouse) and Precision Guided Interventions LLC (spouse); research funding from Instylla (spouse) and Mallinckrodt; patents or royalties with In-Bore LLC; advisory or leadership role on the editorial board of Kidney International Reports, KDIGO Executive Committee, and TriSalus Life Sciences Scientific Advisory Board (spouse); and other interests or relationships include American Society of Pediatric Nephrology Research and Program Committees. B.L. Laskin reports ownership interest in Acorda therapeutics, Charter Communications, Comcast, DHT Holdings, Duke Energy, Electra Battery Materials, Ford Motor, Happiness Development, Johnson Controls, Medtronic, Nu Holdings, AT&T, TE Connectivity, Verizon, and Warner Brothers Discovery; research funding from Viracor Eurofins, research sample testing free of charge; and patent on Compositions and Methods for Treatment of HSCT-Associated Thrombotic Microangiopathy. United States Patent Number PCT/US2014/055922, 2014. J. Zee reports honoraria from Booz Allen Hamilton. All remaining authors have nothing to disclose.
Figures
References
-
- Askenazi DJ Ambalavanan N Hamilton K, et al. Acute kidney injury and renal replacement therapy independently predict mortality in neonatal and pediatric noncardiac patients on extracorporeal membrane oxygenation. Pediatr Crit Care Med. 2011;12(1):e1–e6. doi: 10.1097/PCC.0b013e3181d8e348 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
