

Safety and Outcome of High-Flow Nasal Oxygen Therapy Outside ICU Setting in Hypoxemic Patients With COVID-19
- PMID: 37855812
- PMCID: PMC10715700
- DOI: 10.1097/CCM.0000000000006068
Safety and Outcome of High-Flow Nasal Oxygen Therapy Outside ICU Setting in Hypoxemic Patients With COVID-19
Abstract
Objective: High-flow nasal oxygen (HFNO) therapy is frequently applied outside ICU setting in hypoxemic patients with COVID-19. However, safety concerns limit more widespread use. We aimed to assess the safety and clinical outcomes of initiation of HFNO therapy in COVID-19 on non-ICU wards.
Design: Prospective observational multicenter pragmatic study.
Setting: Respiratory wards and ICUs of 10 hospitals in The Netherlands.
Patients: Adult patients treated with HFNO for COVID-19-associated hypoxemia between December 2020 and July 2021 were included. Patients with treatment limitations were excluded from this analysis.
Interventions: None.
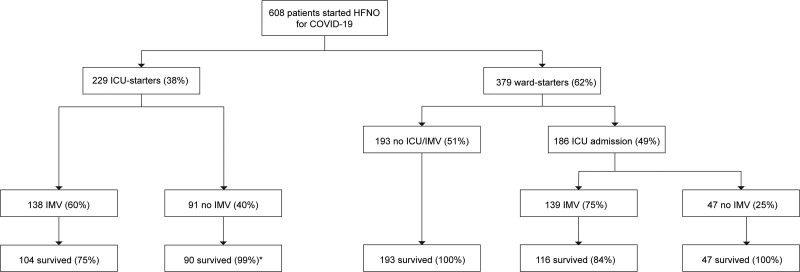
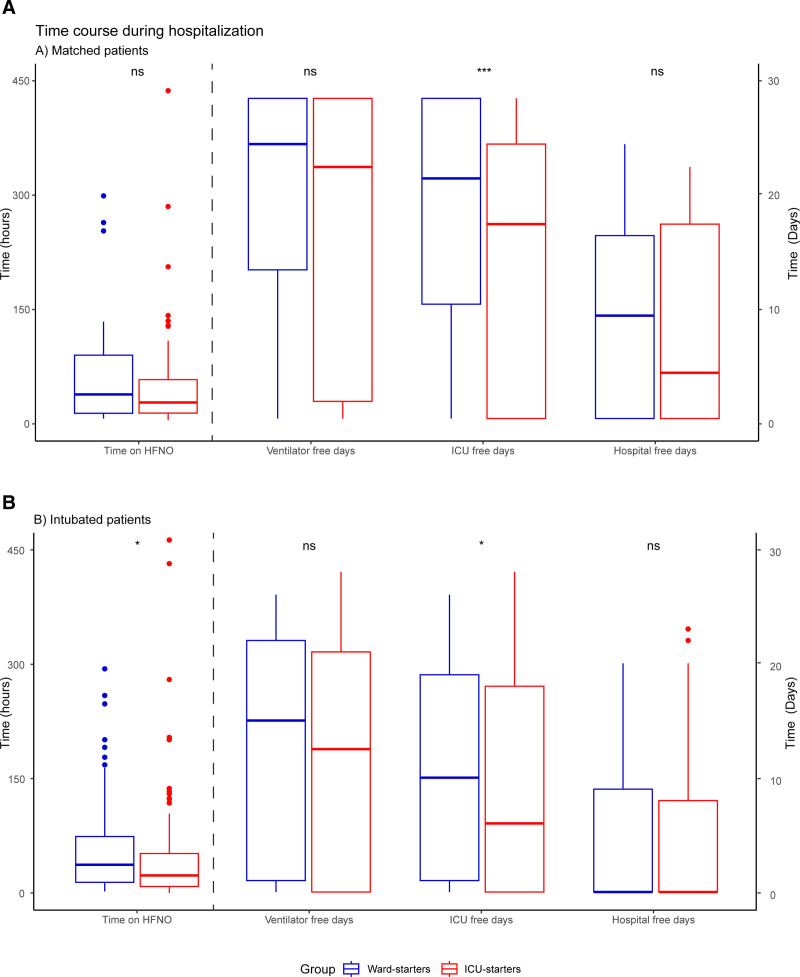
Measurements and main results: Outcomes included intubation and mortality rate, duration of hospital and ICU stay, severity of respiratory failure, and complications. Using propensity-matched analysis, we compared patients who initiated HFNO on the wards versus those in ICU. Six hundred eight patients were included, of whom 379 started HFNO on the ward and 229 in the ICU. The intubation rate in the matched cohort ( n = 214 patients) was 53% and 60% in ward and ICU starters, respectively ( p = 0.41). Mortality rates were comparable between groups (28-d [8% vs 13%], p = 0.28). ICU-free days were significantly higher in ward starters (21 vs 17 d, p < 0.001). No patient died before endotracheal intubation, and the severity of respiratory failure surrounding invasive ventilation and clinical outcomes did not differ between intubated ward and ICU starters (respiratory rate-oxygenation index 3.20 vs 3.38; Pa o2 :F io2 ratio 65 vs 64 mm Hg; prone positioning after intubation 81 vs 78%; mortality rate 17 vs 25% and ventilator-free days at 28 d 15 vs 13 d, all p values > 0.05).
Conclusions: In this large cohort of hypoxemic patients with COVID-19, initiation of HFNO outside the ICU was safe, and clinical outcomes were similar to initiation in the ICU. Furthermore, the initiation of HFNO on wards saved time in ICU without excess mortality or complicated course. Our results indicate that HFNO initiation outside ICU should be further explored in other hypoxemic diseases and clinical settings aiming to preserve ICU capacity and healthcare costs.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Endeman has received unrestricted research grants from Fisher and Paykel Healthcare (Auckland, New Zealand), La Roche Ltd. (Bazel, Switzerland), and Ventinova Medical B.V. (Eindhoven, The Netherlands). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Critical Care Is a Concept, Not a Location.Crit Care Med. 2024 Jan 1;52(1):145-147. doi: 10.1097/CCM.0000000000006086. Epub 2023 Dec 14. Crit Care Med. 2024. PMID: 38095521 No abstract available.
References
-
- Mauri T, Turrini C, Eronia N, et al. : Physiologic Effects of High-Flow Nasal Cannula in Acute Hypoxemic Respiratory Failure. Am J Respir Crit Care Med. 2017; 195:1207–1215 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
