

Robotic-assisted benign hysterectomy compared with laparoscopic, vaginal, and open surgery: a systematic review and meta-analysis
- PMID: 37856058
- PMCID: PMC10678826
- DOI: 10.1007/s11701-023-01724-6
Robotic-assisted benign hysterectomy compared with laparoscopic, vaginal, and open surgery: a systematic review and meta-analysis
Abstract
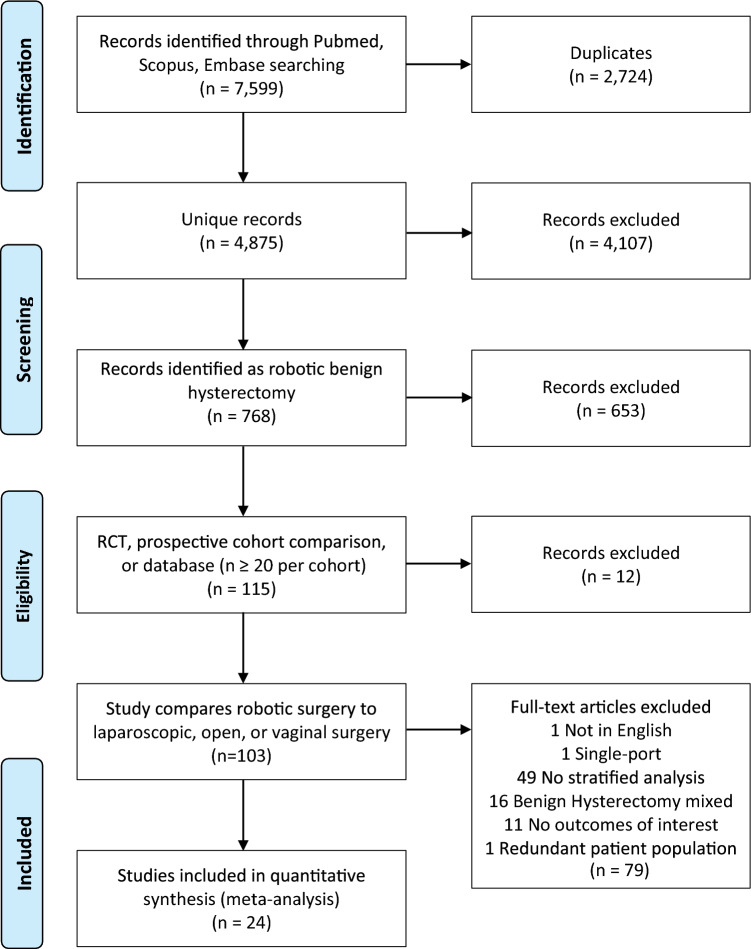
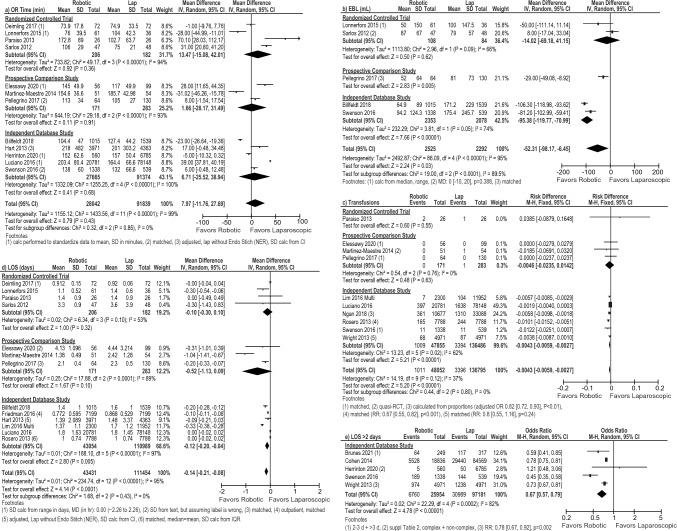
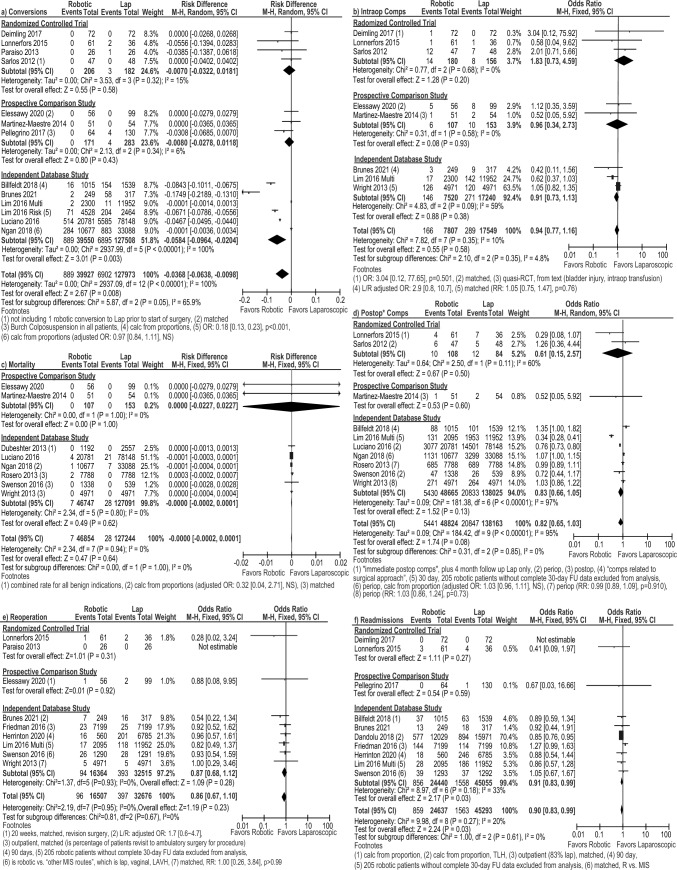
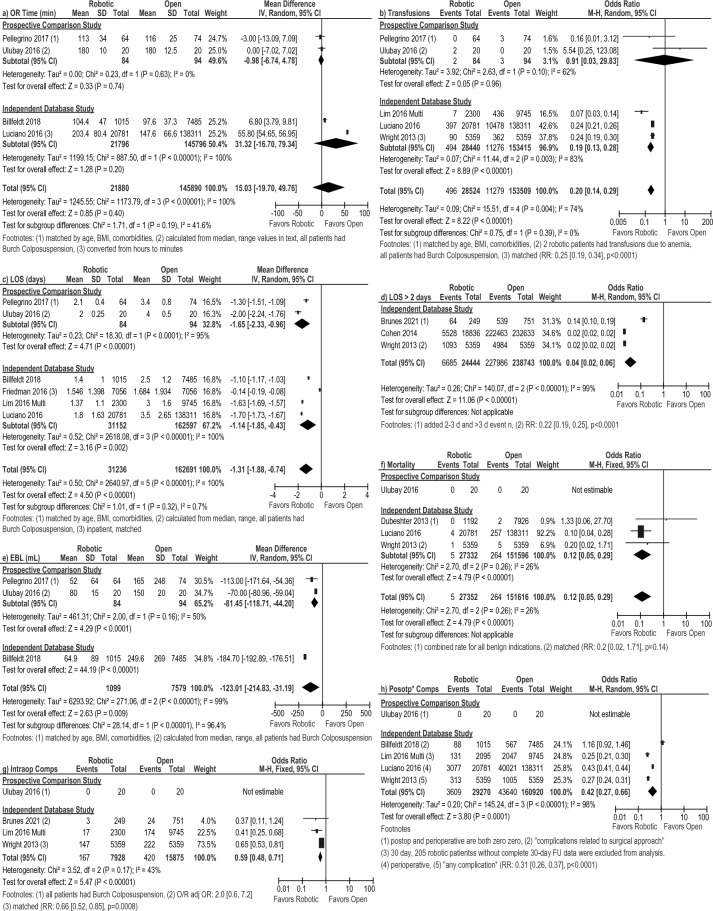
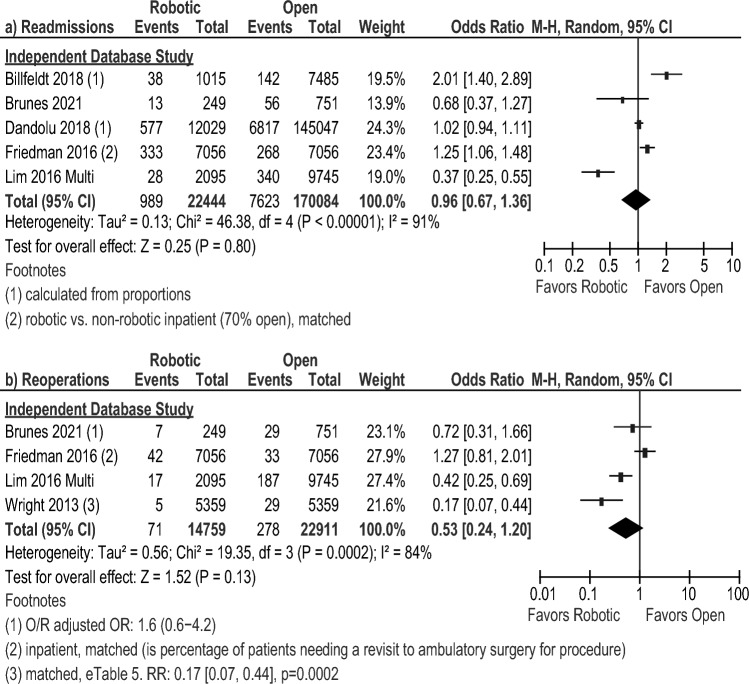
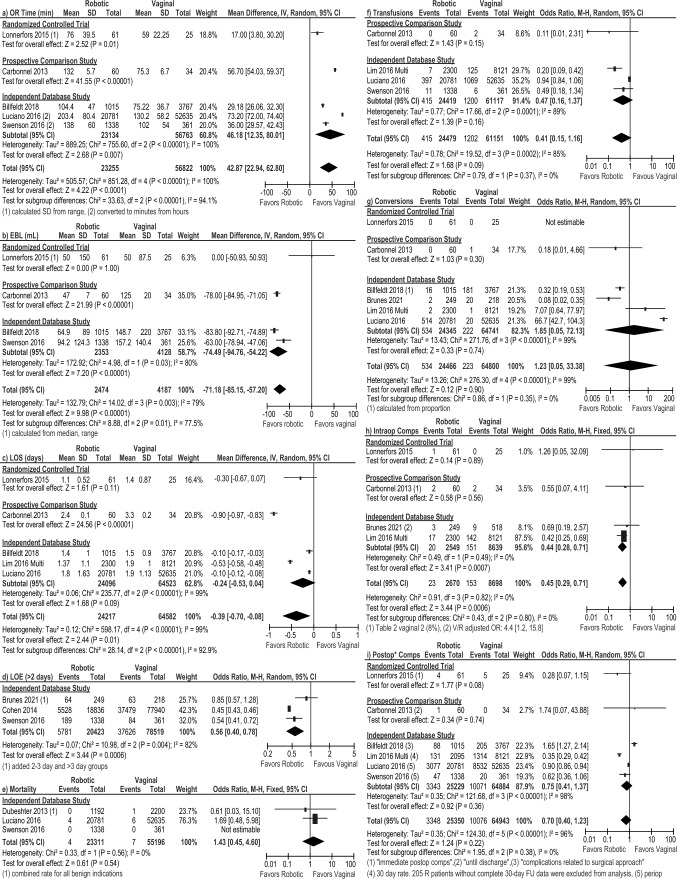
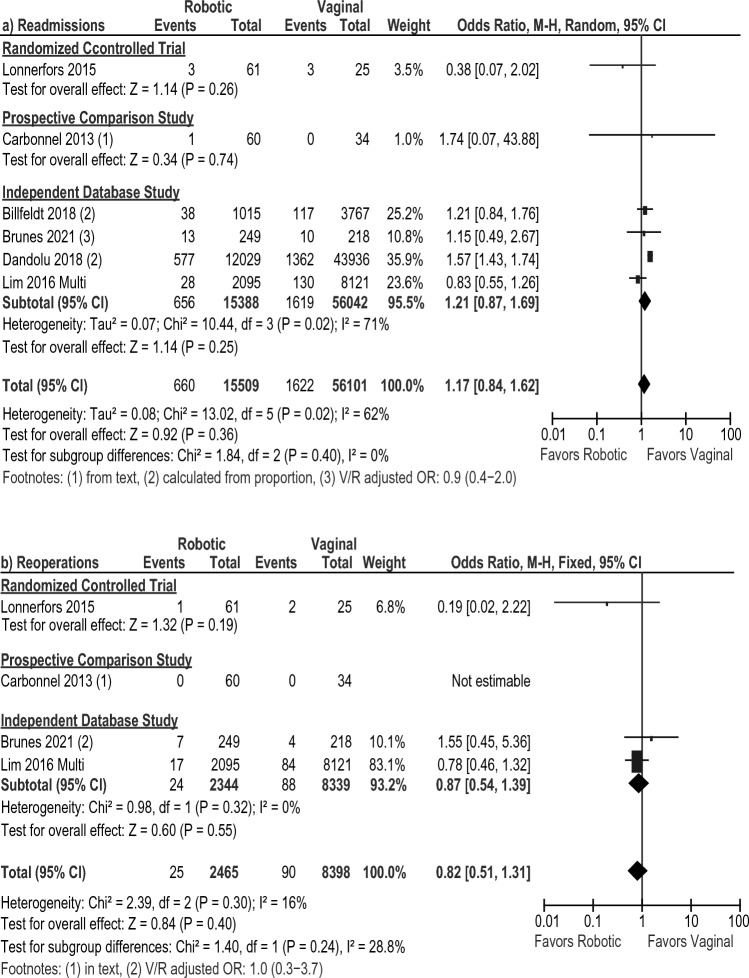
The potential benefits and limitations of benign hysterectomy surgical approaches are still debated. We aimed at evaluating any differences with a systematic review and meta-analysis. PubMed, MEDLINE, and EMBASE databases were last searched on 6/2/2021 to identify English randomized controlled trials (RCTs), prospective cohort and retrospective independent database studies published between Jan 1, 2010 and Dec 31, 2020 reporting perioperative outcomes following robotic hysterectomy versus laparoscopic, open, or vaginal approach (PROSPERO #CRD42022352718). Twenty-four articles were included that reported on 110,306 robotic, 262,715 laparoscopic, 189,237 vaginal, and 554,407 open patients. The robotic approach was associated with a shorter hospital stay (p < 0.00001), less blood loss (p = 0.009), and fewer complications (OR: 0.42 [0.27, 0.66], p = 0.0001) when compared to the open approach. The main benefit compared to the laparoscopic and vaginal approaches was a shorter hospital (R/L WMD: - 0.144 [- 0.21, - 0.08], p < 0.0001; R/V WMD: - 0.39 [- 0.70, - 0.08], p = 0.01). Other benefits seen were sensitive to the inclusion of database studies. Study type differences in outcomes, a lack of RCTs for robotic vs. open comparisons, learning curve issues, and limited robotic vs. vaginal publications are limitations. While the robotic approach was mainly comparable to the laparoscopic approach, this meta-analysis confirms the classic benefits of minimally invasive surgery when comparing robotic hysterectomy to open surgery. We also reported the advantages of robotic surgery over vaginal surgery in a patient population with a higher incidence of large uterus and prior surgery.
Keywords: Benign uterine pathology; Hysterectomy; Laparoscopic hysterectomy; Open hysterectomy; Robotic surgery; Vaginal hysterectomy.
© 2023. The Author(s).
Conflict of interest statement
Pr. Goffroy Canlorbe and Dr. Jérémie Belghiti reported consulting for Intuitive Surgical Inc outside the submitted work. Usha Seshardri Kreaden is an employee of Intuitive Surgical and Dr. April Hebert is a scientific consultant for Intuitive Surgical Inc. Drs. Louis Lenfant, Marianne Nikpayam, Catherine Uzan, and Henri Azaïs have no conflicts of interest or financial ties to disclose.
Figures
References
-
- https://www.has-santefr/upload/docs/application/pdf/2021-12/rapport_hyst.... Accessed 14 Jun 2023
-
- Chevrot A, Margueritte F, Fritel X, Serfaty A, Huchon C, Fauconnier A. Hysterectomy: practices evolution between 2009 and 2019 in France. Gynecol Obstet Fertil Senol. 2021;49:816–822. - PubMed
-
- Gala RB, Margulies R, Steinberg A, Murphy M, Lukban J, Jeppson P, Aschkenazi S, Olivera C, South M, Lowenstein L, Schaffer J, Balk EM, Sung V, Society of Gynecologic Surgeons Systematic Review G Systematic review of robotic surgery in gynecology: robotic techniques compared with laparoscopy and laparotomy. J Minim Invasive Gynecol. 2014;21:353–361. doi: 10.1016/j.jmig.2013.11.010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
