

Improved Cochlear Implant Performance Estimation Using Tonotopic-Based Electrocochleography
- PMID: 37856099
- PMCID: PMC10587831
- DOI: 10.1001/jamaoto.2023.2988
Improved Cochlear Implant Performance Estimation Using Tonotopic-Based Electrocochleography
Abstract
Importance: Cochlear implantation produces remarkable results in postlingual deafness, although auditory outcomes vary. Electrocochleography (ECochG) has emerged as a valuable tool for assessing the cochlear-neural substrate and evaluating patient prognosis.
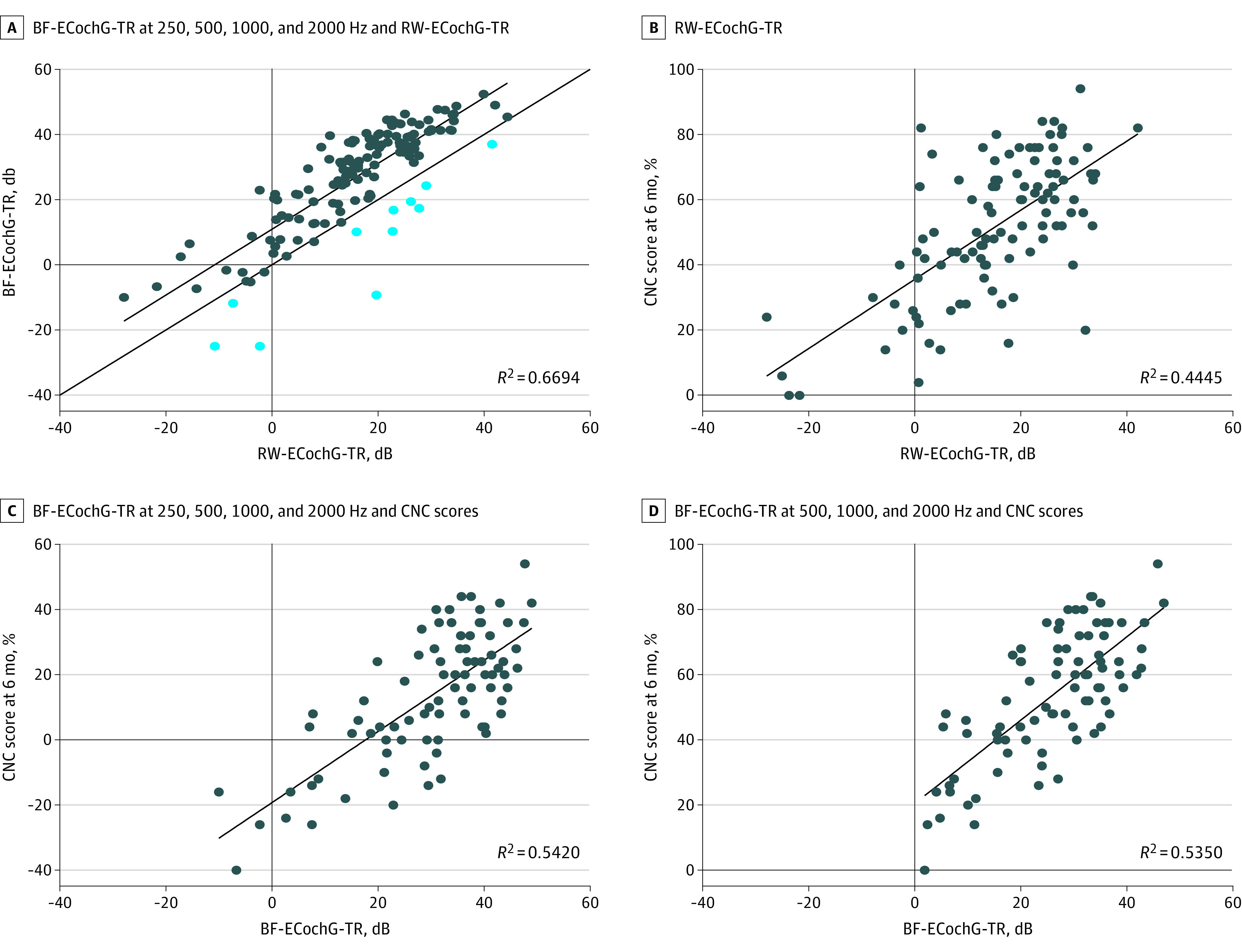
Objective: To assess whether ECochG-total response (ECochG-TR) recorded at the best-frequency electrode (BF-ECochG-TR) correlates more strongly with speech perception performance than ECochG-TR measured at the round window (RW-ECochG-TR).
Design, setting, and participants: This single-center cross-sectional study recruited 142 patients from July 1, 2021, to April 30, 2022, with 1-year follow-up. Exclusions included perilymph suctioning, crimped sound delivery tubes, non-native English speakers, inner ear malformations, nonpatent external auditory canals, or cochlear implantation revision surgery.
Exposures: Cochlear implantation.
Main outcomes and measures: Speech perception testing, including the consonant-nucleus-consonant (CNC) words test, AzBio sentences in quiet, and AzBio sentences in noise plus 10-dB signal to noise ratio (with low scores indicating poor performance and high scores indicating excellent performance on all tests), at 6 months postoperatively; and RW-ECochG-TR and BF-ECochG-TR (measured for 250, 500, 1000, and 2000 Hz).
Results: A total of 109 of the 142 eligible postlingual adults (mean [SD] age, 68.7 [15.8] years; 67 [61.5%] male) were included in the study. Both BF-ECochG-TR and RW-ECochG-TR were correlated with 6-month CNC scores (BF-ECochG-TR: r = 0.74; 95% CI, 0.62-0.82; RW-ECochG-TR: r = 0.67; 95% CI, 0.54-0.76). A multivariate model incorporating age, duration of hearing loss, and angular insertion depth did not outperform BF-ECochG-TR or RW-ECochG-TR alone. The BF-ECochG-TR correlation with CNC scores was significantly stronger than the RW-ECochG-TR correlation (r difference = -0.18; 95% CI, -0.31 to -0.01; z = -2.02). More moderate correlations existed between 6-month AzBio scores in noise, Montreal Cognitive Assessment (MoCA) scores (r = 0.46; 95% CI, 0.29-0.60), and BF-ECochG-TR (r = 0.42; 95% CI, 0.22-0.58). MoCA and the interaction between BF-ECochG-TR and MoCA accounted for a substantial proportion of variability in AzBio scores in noise at 6 months (R2 = 0.50; 95% CI, 0.36-0.61).
Conclusions and relevance: In this case series, BF-ECochG-TR was identified as having a stronger correlation with cochlear implantation performance than RW-ECochG-TR, although both measures highlight the critical role of the cochlear-neural substrate on outcomes. Demographic, audiologic, and surgical factors demonstrated weak correlations with cochlear implantation performance, and performance in noise was found to require a robust cochlear-neural substrate (BF-ECochG-TR) as well as sufficient cognitive capacity (MoCA). Future cochlear implantation studies should consider these variables when assessing performance and related interventions.
Conflict of interest statement
Figures


References
-
- Buchman CA, Gifford RH, Haynes DS, et al. . Unilateral cochlear implants for severe, profound, or moderate sloping to profound bilateral sensorineural hearing loss: a systematic review and consensus statements. JAMA Otolaryngol Head Neck Surg. 2020;146(10):942-953. doi:10.1001/jamaoto.2020.0998 - DOI - PubMed
-
- Zwolan TA, Kallogjeri D, Firszt JB, Buchman CA. Assessment of cochlear implants for adult Medicare beneficiaries aged 65 years or older who meet expanded indications of open-set sentence recognition: a multicenter nonrandomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2020;146(10):933-941. doi:10.1001/jamaoto.2020.2286 - DOI - PMC - PubMed
-
- Rubinstein JT, Parkinson WS, Tyler RS, Gantz BJ. Residual speech recognition and cochlear implant performance: effects of implantation criteria. Am J Otol. 1999;20(4):445-452. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
