

Association of mineral and bone biomarkers with adverse cardiovascular outcomes and mortality in the German Chronic Kidney Disease (GCKD) cohort
- PMID: 37857629
- PMCID: PMC10587182
- DOI: 10.1038/s41413-023-00291-8
Association of mineral and bone biomarkers with adverse cardiovascular outcomes and mortality in the German Chronic Kidney Disease (GCKD) cohort
Abstract
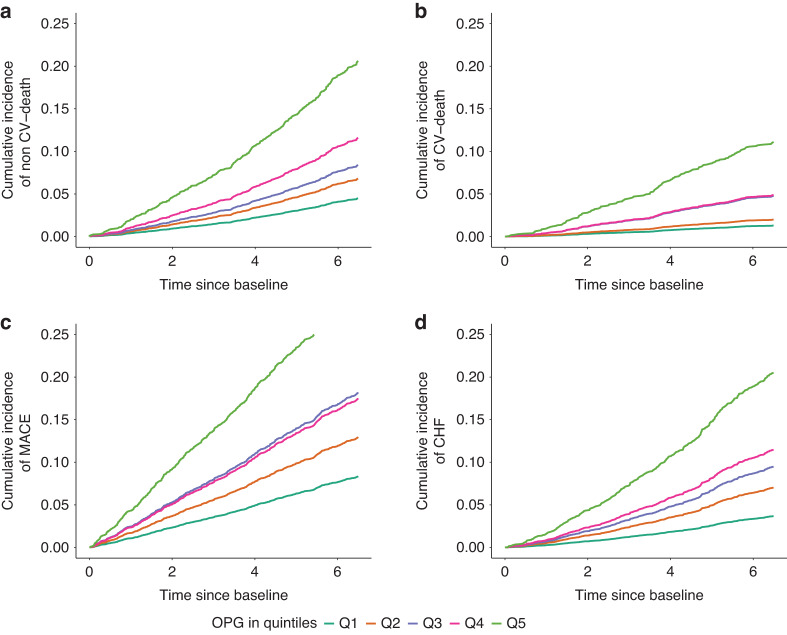
Mineral and bone disorder (MBD) in chronic kidney disease (CKD) is tightly linked to cardiovascular disease (CVD). In this study, we aimed to compare the prognostic value of nine MBD biomarkers to determine those associated best with adverse cardiovascular (CV) outcomes and mortality. In 5 217 participants of the German CKD (GCKD) study enrolled with an estimated glomerular filtration rate (eGFR) between 30-60 mL·min-1 per 1.73 m2 or overt proteinuria, serum osteoprotegerin (OPG), C-terminal fibroblast growth factor-23 (FGF23), intact parathyroid hormone (iPTH), bone alkaline phosphatase (BAP), cross-linked C-telopeptide of type 1 collagen (CTX1), procollagen 1 intact N-terminal propeptide (P1NP), phosphate, calcium, and 25-OH vitamin D were measured at baseline. Participants with missing values among these parameters (n = 971) were excluded, leaving a total of 4 246 participants for analysis. During a median follow-up of 6.5 years, 387 non-CV deaths, 173 CV deaths, 645 nonfatal major adverse CV events (MACEs) and 368 hospitalizations for congestive heart failure (CHF) were observed. OPG and FGF23 were associated with all outcomes, with the highest hazard ratios (HRs) for OPG. In the final Cox regression model, adjusted for CV risk factors, including kidney function and all other investigated biomarkers, each standard deviation increase in OPG was associated with non-CV death (HR 1.76, 95% CI: 1.35-2.30), CV death (HR 2.18, 95% CI: 1.50-3.16), MACE (HR 1.38, 95% CI: 1.12-1.71) and hospitalization for CHF (HR 2.05, 95% CI: 1.56-2.69). Out of the nine biomarkers examined, stratification based on serum OPG best identified the CKD patients who were at the highest risk for any adverse CV outcome and mortality.
© 2023. West China School of Stomatology Sichuan University.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Matsushita K, et al. Epidemiology and risk of cardiovascular disease in populations with chronic kidney disease. Nat. Rev. Nephrol. 2022;18:696–707. - PubMed
-
- Vervloet MG, et al. Bone: a new endocrine organ at the heart of chronic kidney disease and mineral and bone disorders. Lancet Diabetes Endocrinol. 2014;2:427–436. - PubMed
-
- Reiss AB, et al. CKD, arterial calcification, atherosclerosis and bone health: Inter-relationships and controversies. Atherosclerosis. 2018;278:49–59. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
