

The PD-1- and LAG-3-targeting bispecific molecule tebotelimab in solid tumors and hematologic cancers: a phase 1 trial
- PMID: 37857711
- PMCID: PMC10667103
- DOI: 10.1038/s41591-023-02593-0
The PD-1- and LAG-3-targeting bispecific molecule tebotelimab in solid tumors and hematologic cancers: a phase 1 trial
Abstract
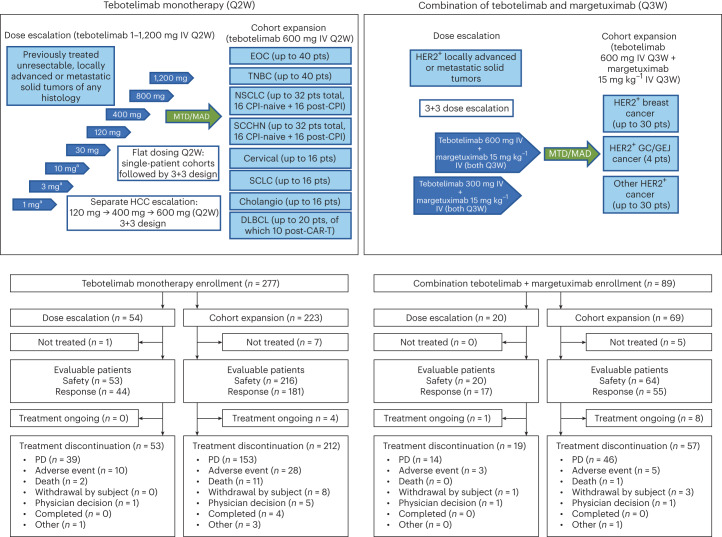
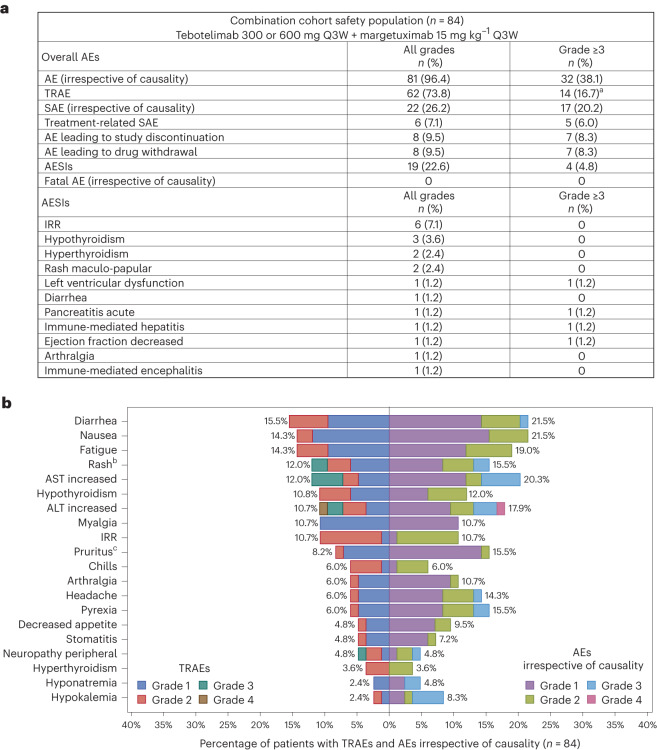
Tebotelimab, a bispecific PD-1×LAG-3 DART molecule that blocks both PD-1 and LAG-3, was investigated for clinical safety and activity in a phase 1 dose-escalation and cohort-expansion clinical trial in patients with solid tumors or hematologic malignancies and disease progression on previous treatment. Primary endpoints were safety and maximum tolerated dose of tebotelimab when administered as a single agent (n = 269) or in combination with the anti-HER2 antibody margetuximab (n = 84). Secondary endpoints included anti-tumor activity. In patients with advanced cancer treated with tebotelimab monotherapy, 68% (184/269) experienced treatment-related adverse events (TRAEs; 22% were grade ≥3). No maximum tolerated dose was defined; the recommended phase 2 dose (RP2D) was 600 mg once every 2 weeks. There were tumor decreases in 34% (59/172) of response-evaluable patients in the dose-escalation cohorts, with objective responses in multiple solid tumor types, including PD-1-refractory disease, and in LAG-3+ non-Hodgkin lymphomas, including CAR-T refractory disease. To enhance potential anti-tumor responses, we tested margetuximab plus tebotelimab. In patients with HER2+ tumors treated with tebotelimab plus margetuximab, 74% (62/84) had TRAEs (17% were grade ≥3). The RP2D was 600 mg once every 3 weeks. The confirmed objective response rate in these patients was 19% (14/72), including responses in patients typically not responsive to anti-HER2/anti-PD-1 combination therapy. ClinicalTrials.gov identifier: NCT03219268 .
© 2023. The Author(s).
Conflict of interest statement
The authors declare the following competing interests. J.J.L. reports grants from AbbVie, Astellas, AstraZeneca, Bristol-Myers Squibb, Corvus, Day One, EMD Serono, Fstar, Genmab, Ikena, Immatics, Incyte, Kadmon, KAHR, MacroGenics, Merck, Moderna, Nektar, Next Cure, Numab, Palleon, Pfizer, Replimmune, Rubius, Servier, Scholar Rock, Synlogic, Takeda, Trishula, Tizona and Xencor; consulting fees from 7 Hills, AbbVie, Actym, Alnylam, Alphamab Oncology, Arch Oncology, Atomwise, Bayer, Bright Peak, Bristol-Myers Squibb, Castle, Checkmate, Codiak, Crown, Cugene, Curadev, Day One, Duke Street Bio, Eisai, EMD Serono, Endeavor, Exo, Flame, Fstar, G1 Therapeutics, Genentech, Gilead, Glenmark, HotSpot, Ikena, Immatics, Immunocore, Incyte, Inzen, Instil, IO Biotech, Janssen, Kadmon, Kanaph, KSQ, MacroGenics, Mavu, Merck, Mersana, Nektar, NeoTx, Novartis, Onc.AI, OncoNano, Partner, Pfizer, Pioneering Medicines, PsiOxus, Pyxis, RefleXion, Regeneron, Ribon, Roivant, Saros, Servier, STINGthera, STipe, Synlogic, Synthekine, Tempest and Xilio; being a member of Data Safety Monitoring Boards for AbbVie, Immutep and Evaxion; leadership role at the Society for Immunotherapy of Cancer; patents (provisional) of serial 15/612,657 (Cancer Immunotherapy), PCT/US18/36052 (Microbiome Biomarkers for Anti-PD-1/PD-L1 Responsiveness: Diagnostic, Prognostic and Therapeutic Uses Thereof); and stock from Actym, Alphamab Oncology, Arch Oncology, Duke Street Bio, Kanaph, Mavu, NeoTx, Onc.AI, OncoNano, Pyxis, Saros, STipe and Tempest. M.R.P. reports leadership of ION Pharma; honoraria from Adaptive Biotechnologies, Bayer, Genentech, Janssen Oncology, Pfizer and Pharmacyclics; consulting for Pharmacyclics/Janssen and Pfizer/EMD Serono; speakers’ bureau for Celgene, Exelixis, Genentech/Roche and Taiho Pharmaceutical; research funding to institution from Acerta Pharma, ADC Therapeutics, Agenus, Aileron Therapeutics, AstraZeneca, BioNTech, Boehringer Ingelheim, Celgene, Checkpoint Therapeutics, CicloMed, Clovis Oncology, Cyteir Therapeutics, Daiichi Sankyo, Eli Lilly, EMD Serono, Evelo Therapeutics, FORMA Therapeutics, Genentech/Roche, Gilead Sciences, GlaxoSmithKline, H3 Biomedicine, Hengrui Therapeutics, Hutchison MediPharma, Ignyta, Incyte, Jacobio, Janssen, Klus Pharma, Kymab, Loxo, LSK Biopartners, Lycera, MacroGenics, Merck, Millennium, Mirati Therapeutics, Moderna Therapeutics, Pfizer, Placon, Portola Pharmaceuticals, Prelude Therapeutics, Ribon Therapeutics, Seven and Eight Biopharmaceuticals, Syndax, Taiho Pharmaceutical, Takeda, Tesaro, TopAlliance BioSciences, Vigeo, ORIC Pharmaceuticals, Puretech, Artios, BioTheryX, Black Diamond Therapeutics, IgM Biosciences, NGM Biopharmaceuticals, Novartis, Nurix, Relay Therapeutics, Samumed, Silicon Therapeutics, TeneoBio, Treadwell Therapeutics, Zymeworks, Olema, Adagene, Astellas, Accutar Biotech, TeneoBio, Compugen, MabSpace Biosciences, Immunogen and Blueprint Pharmaceuticals. G.B. reports grant/contract for clinical trial from MacroGenics; grants from Amgen, Bayer, Adaptimmune, Exelixis, Daiichi Sankyo, GlaxoSmithKline, Immatics, Immunocore, Incyte, Kite Pharma, MacroGenics, Torque, AstraZeneca, Bristol-Myers Squibb, Celgene, Genentech, MedImmune, Merck, Novartis, Roche, Sanofi, Xcovery, Tmunity Therapeutics, Regeneron, BeiGene, Repertoire Immune Medicines, Verastem, CytomX Therapeutics and Duality Biologics; consulting fees from AbbVie, Adicet, Amgen, Ariad, Bayer, Clovis Oncology, AstraZeneca, Bristol-Myers Squibb, Celgene, Daiichi Sankyo, Instil Bio, Genentech, Genzyme, Gilead, Eli Lilly, Janssen, MedImmune, Merck, Novartis, Roche, Sanofi, Tyme Oncology, Xcovery, Virogin Biotech, Maverick Therapeutics, BeiGene, Regeneron, Cytomx Therapeutics, Intervenn Biosciences and Onconova Therapeutics; participation in advisory boards at Virogin Biotech SAB and Maverick Therapeutics SAB; stock in Virogin Biotech; and employment of family member at Johnson & Johnson/Janssen. E.H. reports grant/contract for clinical trial from MacroGenics; grants to institution from AbbVie, Acerta Pharma, Accutar Biotechnology, ADC Therapeutics, AKESOBIO Australia, Amgen, Aravive, Artios, Arvinas, AstraZeneca, AtlasMedx, BeiGene, Black Diamond Therapeutics, Bliss BioPharmaceuticals, Boehringer Ingelheim, Cascadian Therapeutics, Clovis, Compugen, Cullinan-Florentine, Curis, CytomX, Daiichi Sankyo, Danatari, Deciphera, Duality Biologics, eFFECTOR Therapeutics, Ellipses Pharma, Elucida Oncology, EMD Serono, FujiFilm, G1 Therapeutics, H3 Biomedicine, Harpoon, Hutchinson MediPharma, Immunogen, Immunomedics, Incyte, Infinity Pharmaceuticals, InvestisBio, Jacobio, Karyopharm, K-Group Beta, Leap Therapeutics, Eli Lilly, Loxo Oncology, Lycera, MabSpace Biosciences, MacroGenics, MedImmune, Mersana, Merus, Millennium, Molecular Templates, Novartis, Nucana, Olema, OncoMed, Onconova Therapeutics, Oncothyreon, ORIC Pharmaceuticals, Orinove, Pfizer, PharmaMar, Pieris Pharmaceuticals, Pionyr Immunotherapeutics, Plexxikon, Radius Health, Regeneron, Relay Therapeutics, Repertoire Immune Medicine, Rgenix, Roche/Genentech, SeaGen, Sermonix Pharmaceuticals, Shattuck Labs, StemCentRx, Sutro, Syndax, Syros, Taiho, TapImmune, Tesaro, Tolmar, Torque Therapeutics, Treadwell Therapeutics, Verastem, Vincerx Pharma, Zenith Epigenetics and Zymeworks; and consulting fees to institution from Arcus, Arvinas, AstraZeneca, Daiichi Sankyo, Deciphera Pharmaceuticals, Ellipses Pharma, Greenwich LifeSciences, iTeos, Janssen, Eli Lilly, Loxo, Mersana, Novartis, Orum Therapeutics, Pfizer, Relay Therapeutics, Roche/Genentech, SeaGen and Verascity Science. B.C. reports grants from Bristol-Myers Squibb, MacroGenics, Merck, Karyopharm Therapeutics, Infinity Pharmaceuticals, Advenchen Laboratories, Idera, Xencor, Compugen, Iovance Biotherapeutics, PACT Pharma, RAPT Therapeutics, Immunocore, IDEAYA Biosciences, Ascentage Pharma, Novartis, Atreca, Replimune, Instil Bio, Adagene and TriSalus Life Sciences; consulting fees from IDEAYA Biosciences, OncoSec, Genentech, Novartis, Delcath Systems and Instil Bio; and participation in advisory board at Nektar. S.V.U. reports grants to institution from AbbVie, ArQule, AstraZeneca, Atreca, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Ciclomed, Evelo Biosciences, Exelixis, G1 Therapeutics, GlaxoSmithKline, Hutchmed, IGM Biosciences, Incyte, Isofol, Klus Pharma, MacroGenics, Merck, Mersana Therapeutics, OncoMed Pharmaceuticals, Pfizer, Regeneron, Revolution Medicines, Synermore Biologics, Takeda, Tarveda Therapeutics, Tesaro, Tempest and Vigeo Therapeutics and participation in advisory boards at Array, Incyte, Bayer, Syros, Eisai and Exelixis. R.M.C. reports grants to institution from Pfizer, MSD Ireland, Daiichi Sankyo and AstraZeneca; participation at Data Safety Monitoring Boards for the HER2 RADiCAL study of the NIHR UK, the DECRESCENDO trial of the Breast International Group and the SAB UCD Cancer Trials Group; participation in advisory board as chair at Seagen; and consulting for Seagen, AstraZeneca and Daiichi Sankyo. C.A.S-M. reports advisory board with honoraria from Seattle Genetics, Genomic Health and Athenex and advisory board without honoraria from Merck, Pfizer and Bristol-Myers Squibb. J.W. reports advisory board at Kyowa Kirin. A.W. reports grant from Merck and advisory boards at Merck Serono, Merck and Bristol-Myers Squibb. N.H. reports advisory board with honoraria from Novartis, AbbVie, Roche, Janssen, Takeda, Pfizer, Amgen and Jazz Pharmaceuticals. H.L.K. reports consulting fees from AstraZeneca, Bluestar Genomics, Deciphera, Novocure, Sanofi and Tempus. B.J.S. reports stock options as a condition of employment at MacroGenics; patents planned, issued or pending for WO2021133653 and WO2022026306, with MacroGenics—counterpart applications have been filed worldwide; and funding for the present manuscript as the sponsor from MacroGenics. P.K. reports stock options as a condition of employment at MacroGenics and patents planned, issued or pending for WO2016200782, WO2017019846, WO2021133653 and WO2022026306 with MacroGenics—counterpart applications have been filed worldwide. F.Z.C. reports stock options as a condition of employment at MacroGenics and funding for the present manuscript from MacroGenics. X.Z. reports stock options as a condition of employment at MacroGenics; patents planned, issued or pending for WO2021133653, with MacroGenics; and funding for the present manuscript from MacroGenics. K.S. reports stock options as a condition of employment at MacroGenics; patents planned, issued or pending for WO201620078 and WO2017019846, with MacroGenics; and funding for the present manuscript from MacroGenics. D.H.S. reports stock options as a condition of employment at MacroGenics; patents planned, issued or pending for WO2016200782 and WO2017019846, with MacroGenics; and funding for the present manuscript from MacroGenics. A.D.C. reports stock options as a condition of employment at MacroGenics and funding for the present manuscript from MacroGenics. J.L. reports stock options as a condition of employment at MacroGenics and funding for the present manuscript from MacroGenics. H.L. reports stock options as a condition of employment at MacroGenics and funding for the present manuscript from MacroGenics. J.S. is a former employee of MacroGenics and reports stock options as a condition of past employment at MacroGenics. J.S. also reports funding for the present manuscript from MacroGenics. P.A.M. is a former employee of MacroGenics and reports stock options as a condition of past employment at MacroGenics; patents planned, issued or pending for WO2016200782, WO2017019846, WO2021133653 and WO2022026306, with MacroGenics—counterpart applications have been filed worldwide; and funding for the present manuscript as the sponsor from MacroGenics. These authors declare no competing interests: S.W.B., G.M., A.S.A, P.C., M.D.-D., M.T.-K. and H.P.
Figures









References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
