

Maturation of cardioventilatory physiological trajectories in extremely preterm infants
- PMID: 37857848
- PMCID: PMC11580183
- DOI: 10.1038/s41390-023-02839-0
Maturation of cardioventilatory physiological trajectories in extremely preterm infants
Abstract
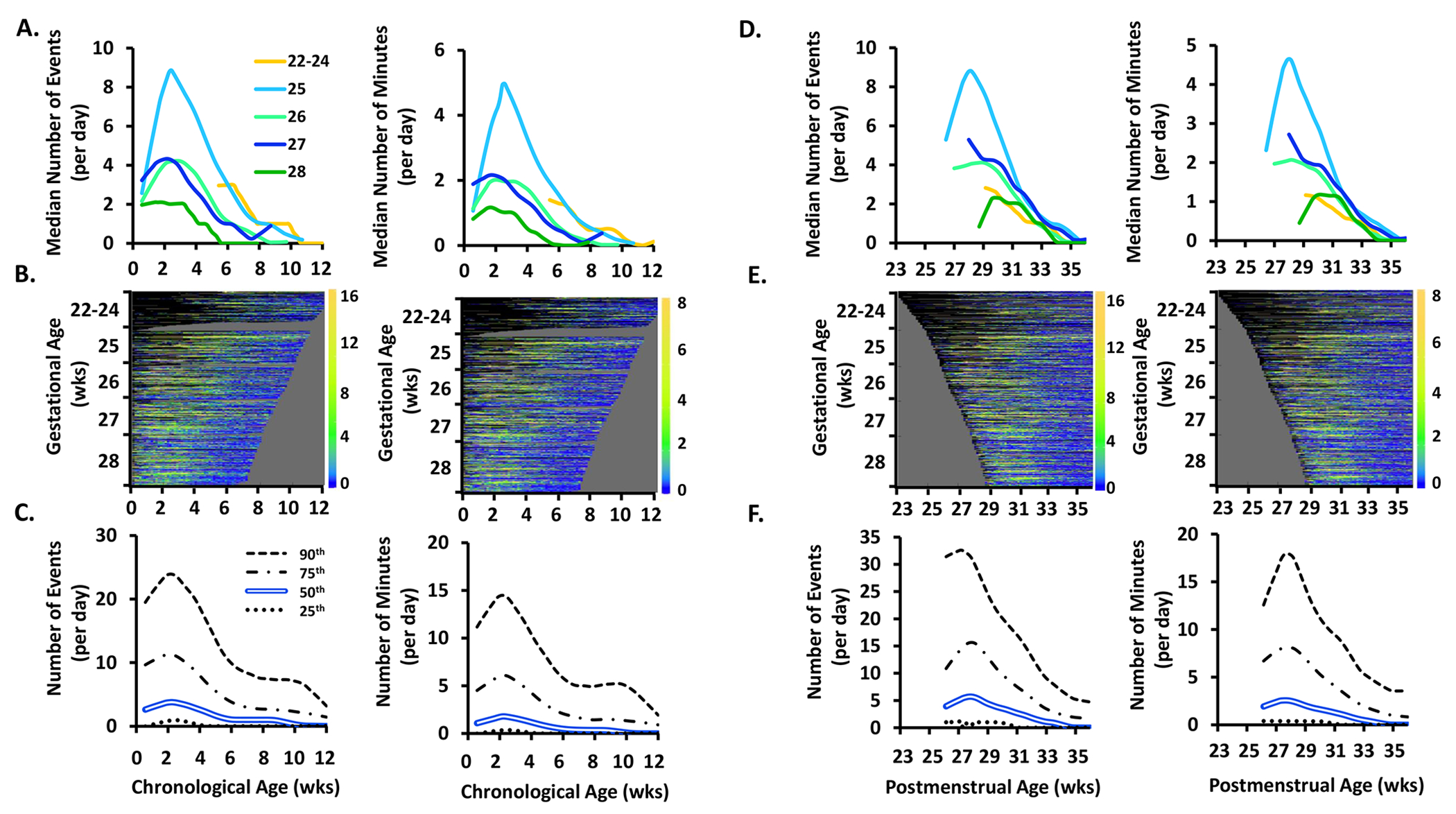
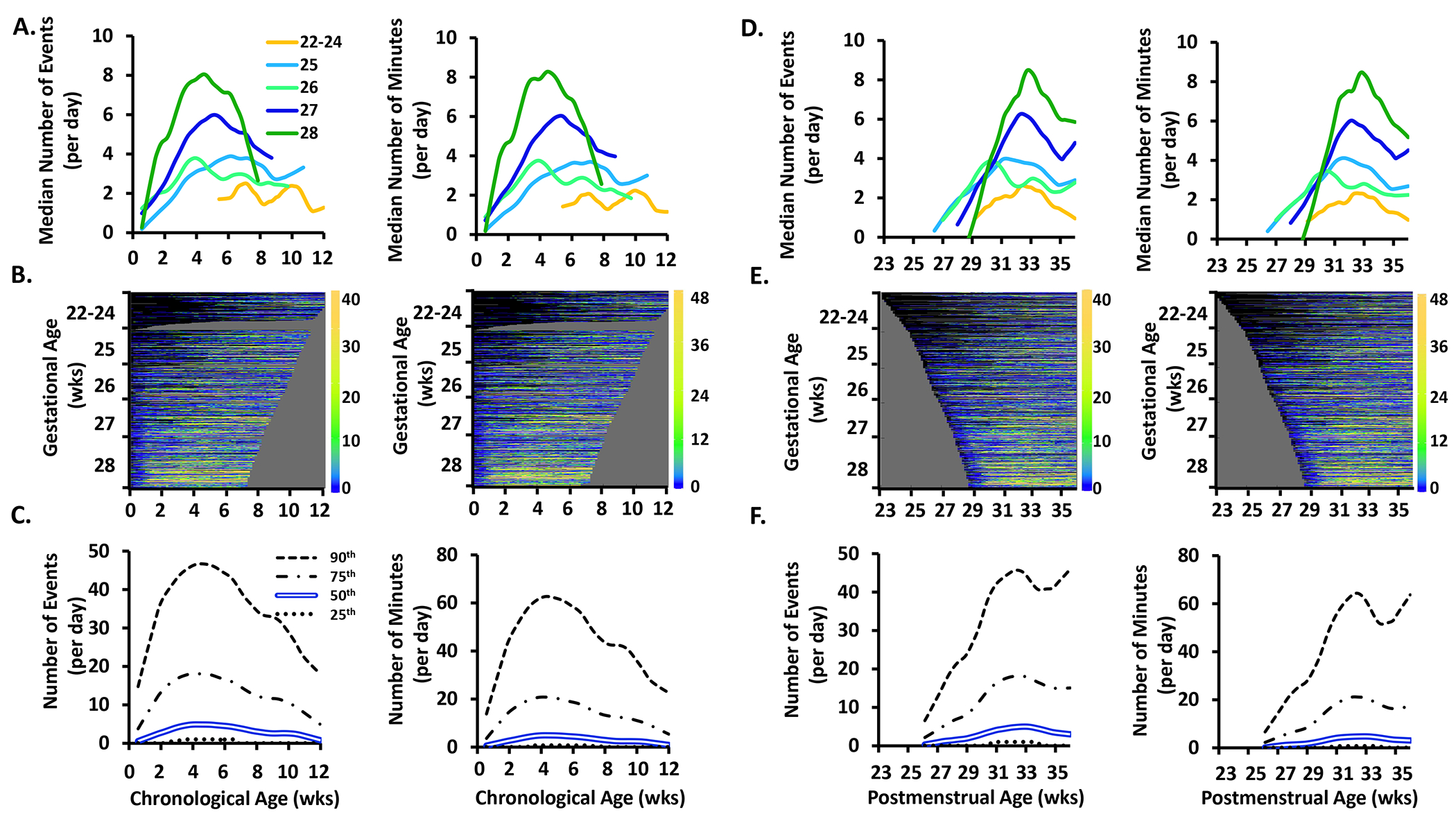
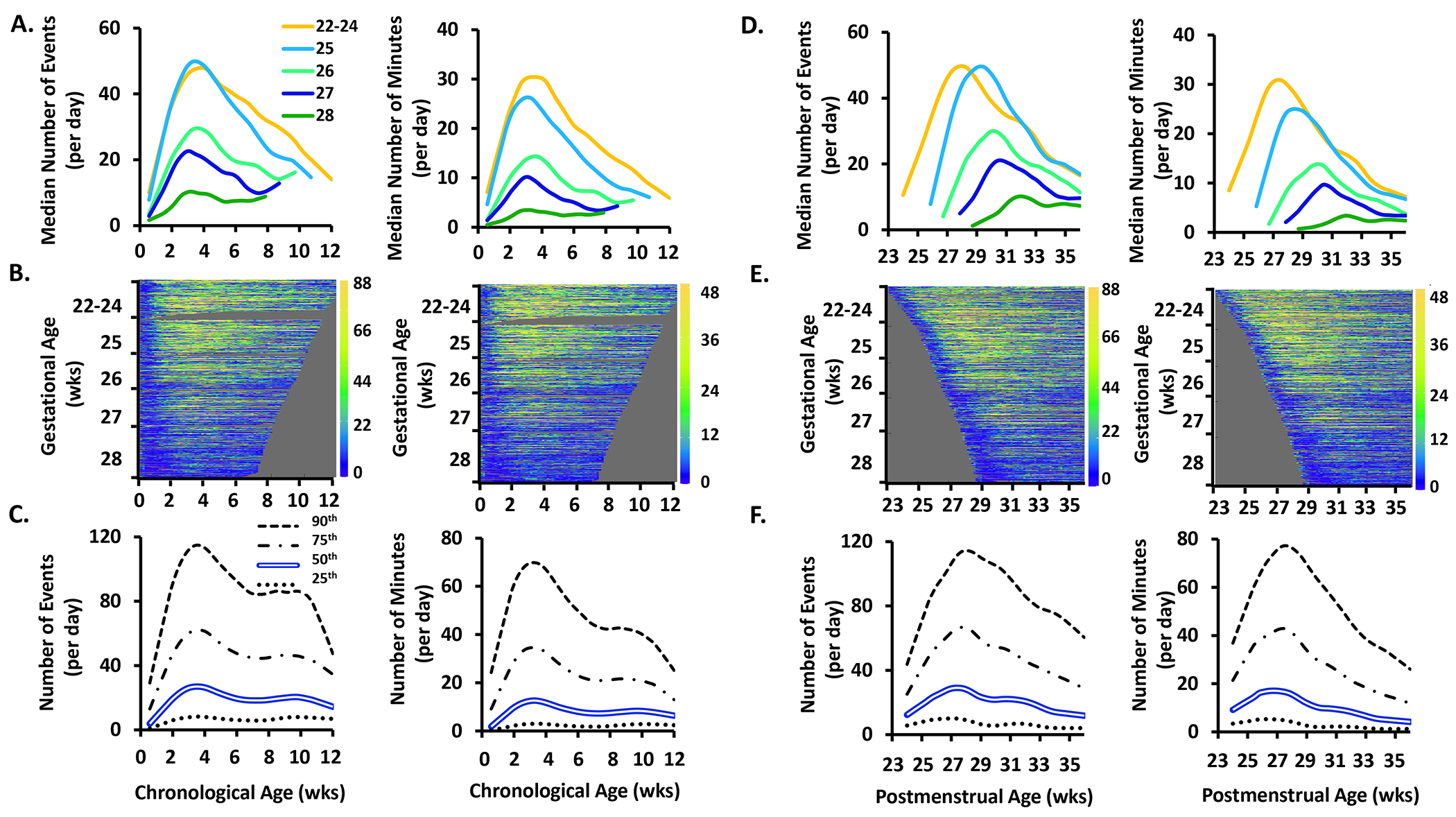
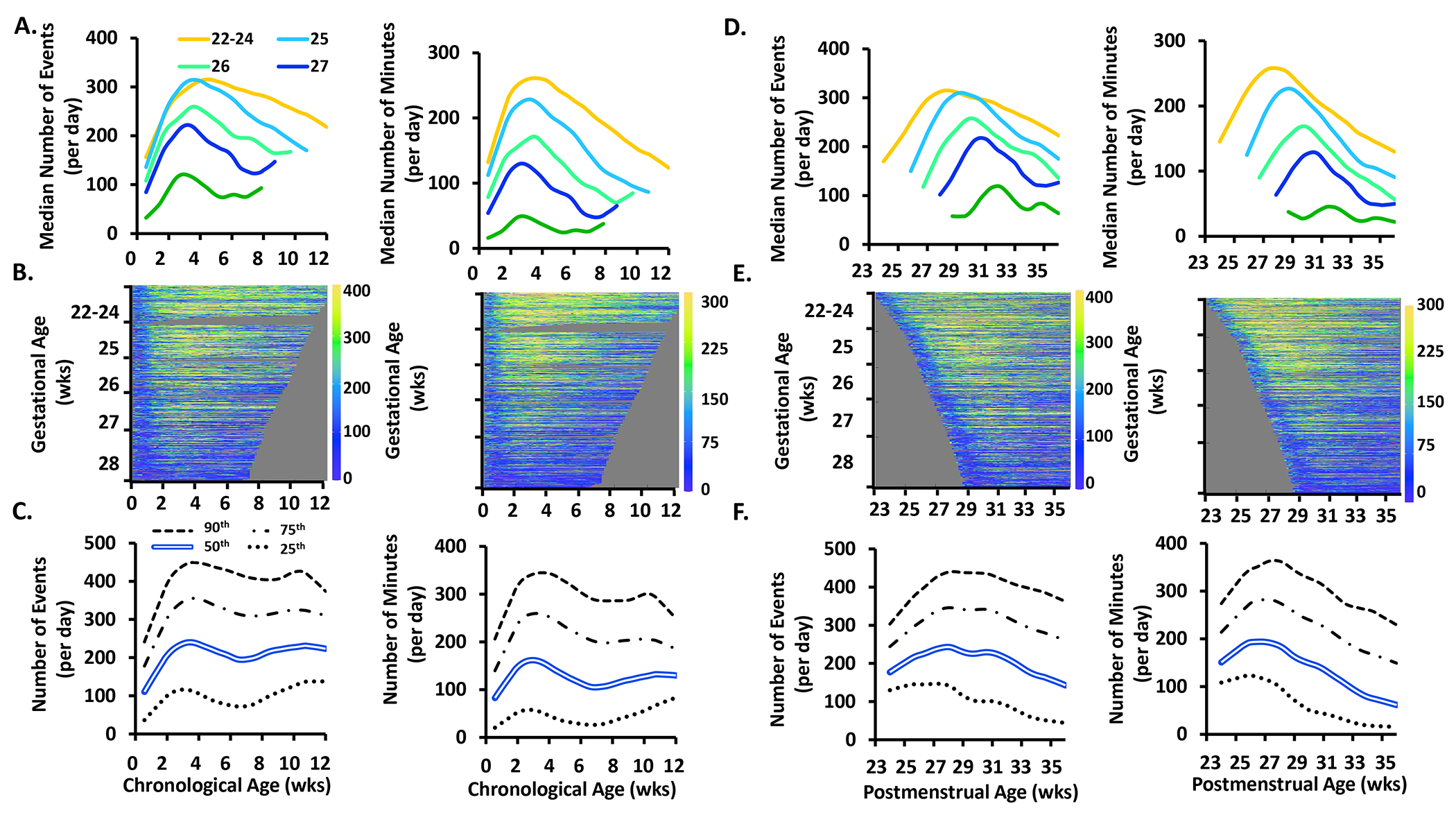
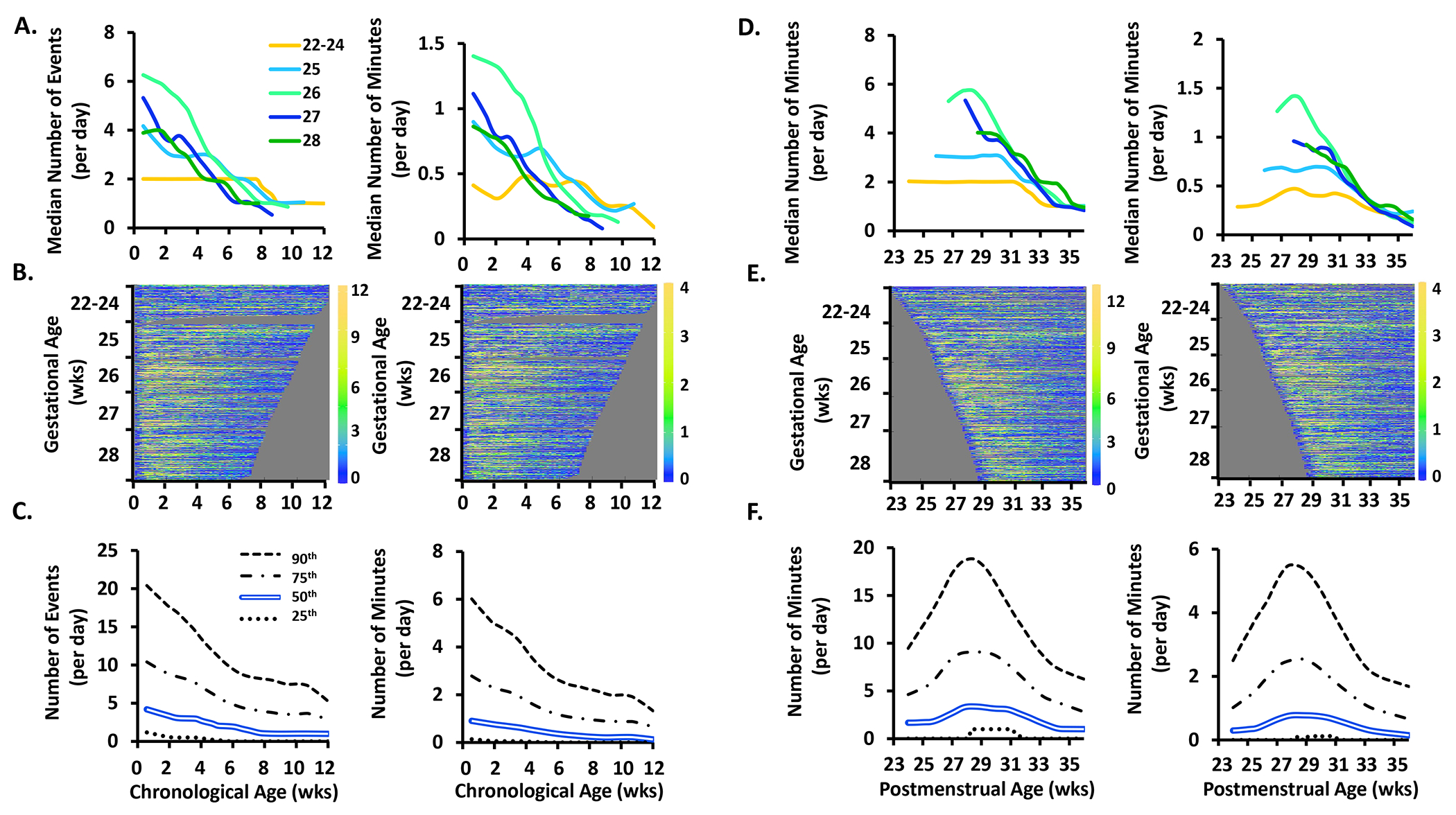
Background: In extremely preterm infants, persistence of cardioventilatory events is associated with long-term morbidity. Therefore, the objective was to characterize physiologic growth curves of apnea, periodic breathing, intermittent hypoxemia, and bradycardia in extremely preterm infants during the first few months of life.
Methods: The Prematurity-Related Ventilatory Control study included 717 preterm infants <29 weeks gestation. Waveforms were downloaded from bedside monitors with a novel sharing analytics strategy utilized to run software locally, with summary data sent to the Data Coordinating Center for compilation.
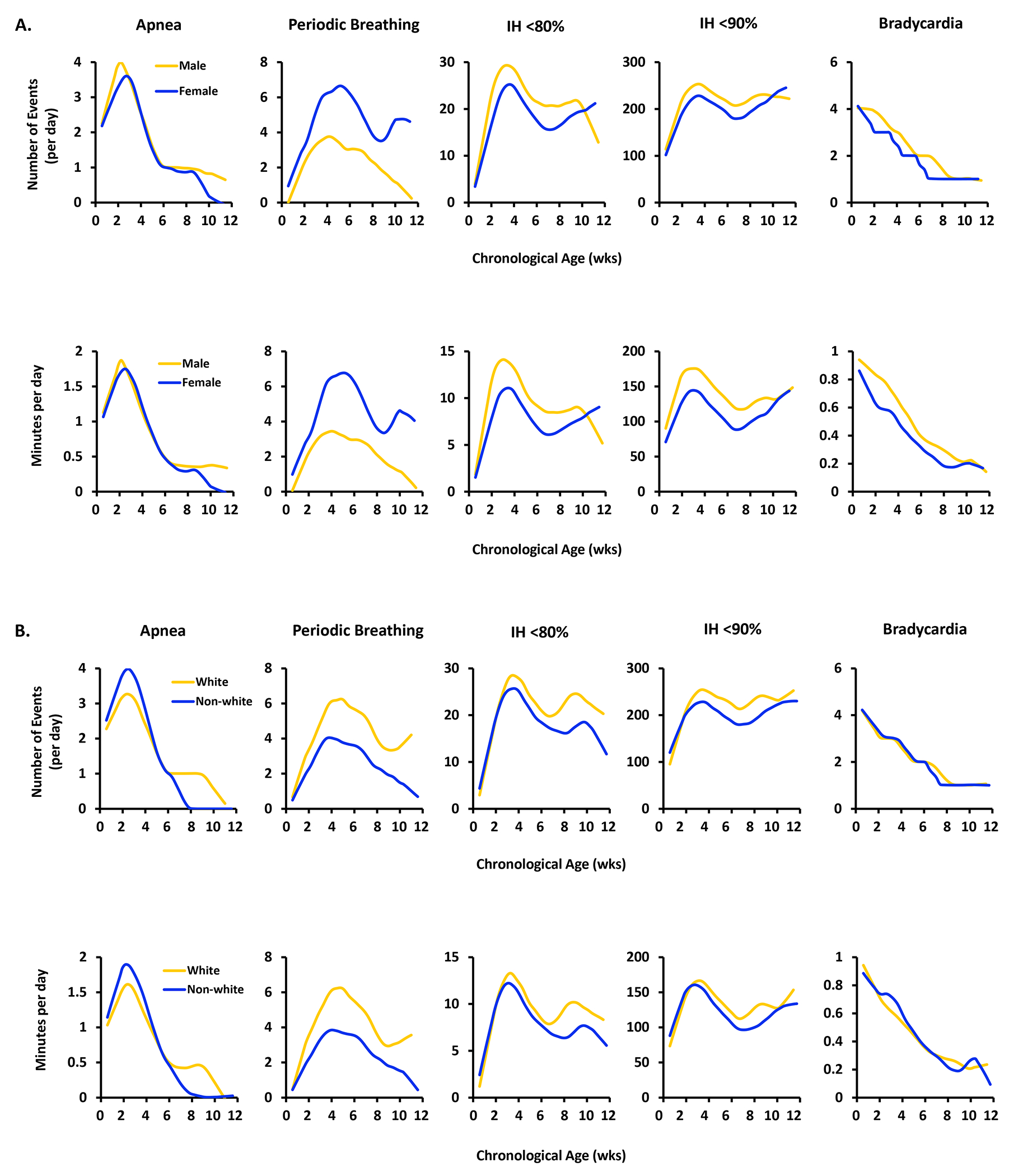
Results: Apnea, periodic breathing, and intermittent hypoxemia events rose from day 3 of life then fell to near-resolution by 8-12 weeks of age. Apnea/intermittent hypoxemia were inversely correlated with gestational age, peaking at 3-4 weeks of age. Periodic breathing was positively correlated with gestational age peaking at 31-33 weeks postmenstrual age. Females had more periodic breathing but less intermittent hypoxemia/bradycardia. White infants had more apnea/periodic breathing/intermittent hypoxemia. Infants never receiving mechanical ventilation followed similar postnatal trajectories but with less apnea and intermittent hypoxemia, and more periodic breathing.
Conclusions: Cardioventilatory events peak during the first month of life but the actual postnatal trajectory is dependent on the type of event, race, sex and use of mechanical ventilation.
Impact: Physiologic curves of cardiorespiratory events in extremely preterm-born infants offer (1) objective measures to assess individual patient courses and (2) guides for research into control of ventilation, biomarkers and outcomes. Presented are updated maturational trajectories of apnea, periodic breathing, intermittent hypoxemia, and bradycardia in 717 infants born <29 weeks gestation from the multi-site NHLBI-funded Pre-Vent study. Cardioventilatory events peak during the first month of life but the actual postnatal trajectory is dependent on the type of event, race, sex and use of mechanical ventilation. Different time courses for apnea and periodic breathing suggest different maturational mechanisms.
© 2023. The Author(s), under exclusive licence to the International Pediatric Research Foundation, Inc.
Conflict of interest statement
Figures
References
-
- Poets CF et al. Association Between Intermittent Hypoxemia or Bradycardia and Late Death or Disability in Extremely Preterm Infants. JAMA. 314,595–603(2015). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
