

A score to predict Pseudomonas aeruginosa infection in older patients with community-acquired pneumonia
- PMID: 37858082
- PMCID: PMC10585923
- DOI: 10.1186/s12879-023-08688-w
A score to predict Pseudomonas aeruginosa infection in older patients with community-acquired pneumonia
Abstract
Background: In Thailand, the incidence of community-acquired pseudomonal pneumonia among 60- to 65-year-olds ranges from 10.90% to 15.51%, with a mortality rate of up to 19.00%. Antipseudomonal agents should be selected as an empirical treatment for elderly patients at high risk for developing this infection. The purpose of this study was to identify risk factors and develop a risk predictor for Pseudomonas aeruginosa infection in older adults with community-acquired pneumonia (CAP).
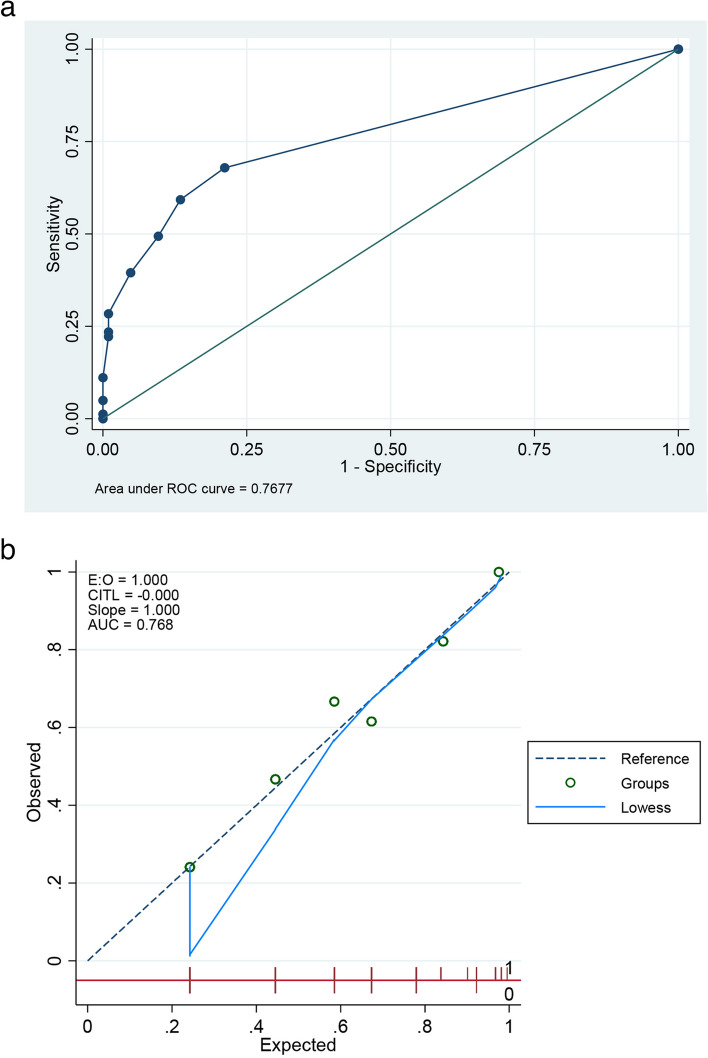
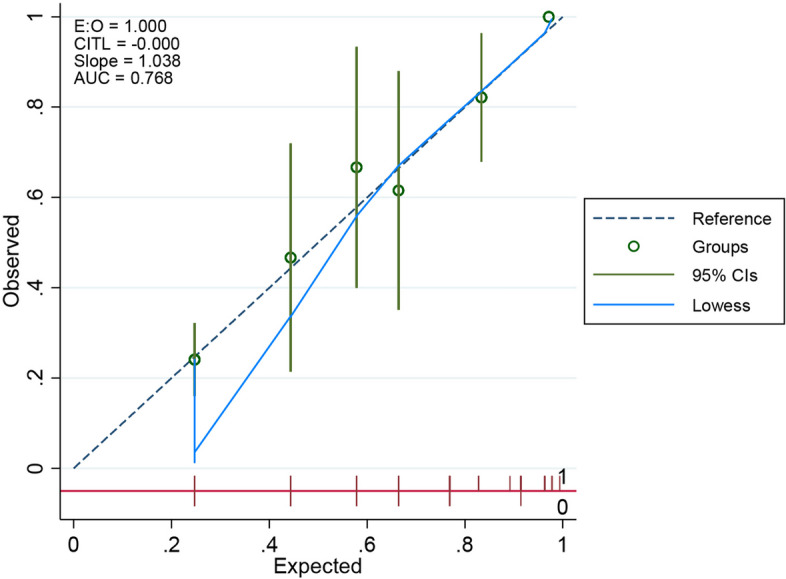
Methods: A retrospective data collection from an electronic database involved the elderly hospitalized patients with P. aeruginosa- and non-P. aeruginosa-causing CAP, admitted between January 1, 2016, and June 30, 2021. Risk factors for P. aeruginosa infection were analysed using logistic regression, and the instrument was developed by scoring each risk factor based on the beta coefficient and evaluating discrimination and calibration using the area under the receiver operating characteristic curve (AuROC) and observed versus predicted probability (E/O) ratio.
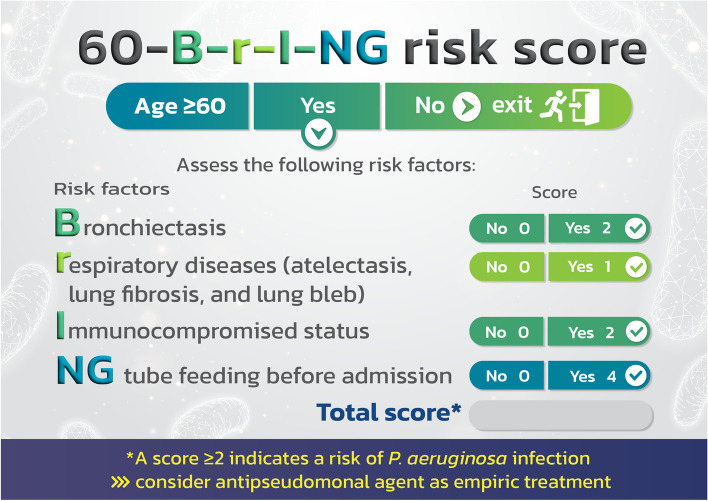
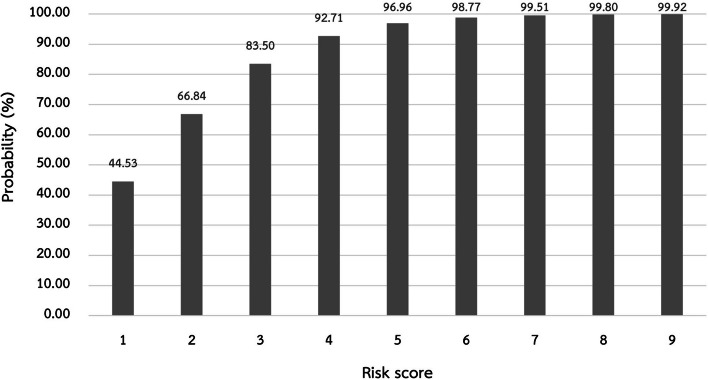
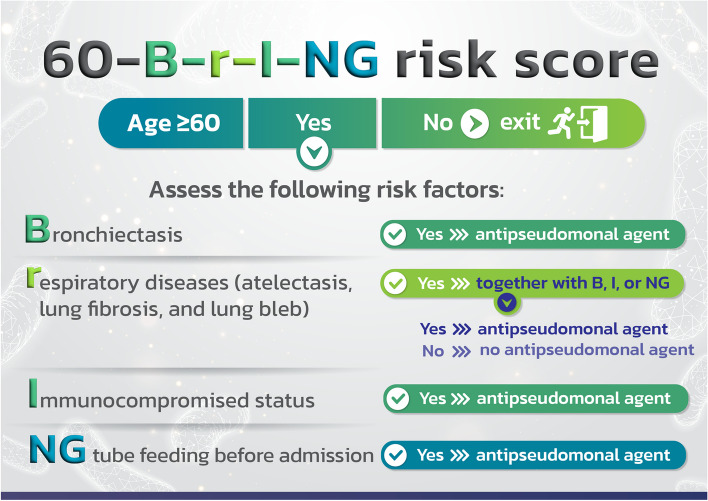
Results: The inclusion criteria were met by 81 and 104 elderly patients diagnosed with CAP caused by P. aeruginosa and non-P. aeruginosa, respectively. Nasogastric (NG) tube feeding (odd ratios; OR = 40.68), bronchiectasis (B) (OR = 4.13), immunocompromised condition (I) (OR = 3.76), and other chronic respiratory illnesses (r) such as atelectasis, pulmonary fibrosis, and lung bleb (OR = 2.61) were the specific risk factors for infection with P. aeruginosa. The "60-B-r-I-NG" risk score was named after the 4 abbreviated risk variables and found to have good predicative capability (AuROC = 0.77) and accuracy comparable to or near true P. aeruginosa infection (E/O = 1). People who scored at least two should receive empirically antipseudomonal medication.
Conclusions: NG tube feeding before admission, bronchiectasis, immunocompromisation, atelectasis, pulmonary fibrosis and lung bleb were risk factors for pseudomonal CAP in the elderly. The 60-B-r-I-NG was developed for predicting P. aeruginosa infection with a high degree of accuracy, equal to or comparable to the existing P. aeruginosa infection. Antipseudomonal agents may be started in patients who are at least 60 years old and have a score of at least 2 in order to lower mortality and promote the appropriate use of these medications.
Keywords: Community-acquired pneumonia; Elderly; P. aeruginosa; Predictive risk score.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Determinants of empirical antipseudomonal antibiotic prescription for adults with pneumonia in the emergency department.BMC Pulm Med. 2020 Apr 3;20(1):83. doi: 10.1186/s12890-020-1115-0. BMC Pulm Med. 2020. PMID: 32245452 Free PMC article.
-
Risk factors and antibiotic therapy in P. aeruginosa community-acquired pneumonia.Respirology. 2015 May;20(4):660-6. doi: 10.1111/resp.12506. Epub 2015 Mar 16. Respirology. 2015. PMID: 25776134
-
[Chinese expert consensus on the management of lower respiratory tract infections of Pseudomonas aeruginosa in adults(2022)].Zhonghua Jie He He Hu Xi Za Zhi. 2022 Aug 12;45(8):739-752. doi: 10.3760/cma.j.cn112147-20220407-00290. Zhonghua Jie He He Hu Xi Za Zhi. 2022. PMID: 35927044 Chinese.
-
The treatment of respiratory pseudomonas infection in cystic fibrosis: what drug and which way?Drugs. 2000 Nov;60(5):1053-64. doi: 10.2165/00003495-200060050-00006. Drugs. 2000. PMID: 11129122 Review.
-
Pseudomonas aeruginosa pneumonia.Curr Opin Infect Dis. 2003 Apr;16(2):135-43. doi: 10.1097/00001432-200304000-00010. Curr Opin Infect Dis. 2003. PMID: 12734446 Review.
Cited by
-
Molecular Properties of Virulence and Antibiotic Resistance of Pseudomonas aeruginosa Causing Clinically Critical Infections.Pathogens. 2024 Oct 3;13(10):868. doi: 10.3390/pathogens13100868. Pathogens. 2024. PMID: 39452738 Free PMC article.
-
Development and Validation of a Nomogram for Predicting Multidrug-Resistant Pseudomonas Aeruginosa Pneumonia in Hospitalized Patients.Infect Drug Resist. 2025 Jul 16;18:3543-3559. doi: 10.2147/IDR.S527949. eCollection 2025. Infect Drug Resist. 2025. PMID: 40689220 Free PMC article.
-
Enhancing prognostic prediction of invasive candidiasis among cancer patients with a serum C5a-based scoring model.Support Care Cancer. 2024 May 15;32(6):356. doi: 10.1007/s00520-024-08567-3. Support Care Cancer. 2024. PMID: 38750396
-
Antibiotic Resistance in the Elderly: Mechanisms, Risk Factors, and Solutions.Microorganisms. 2024 Sep 30;12(10):1978. doi: 10.3390/microorganisms12101978. Microorganisms. 2024. PMID: 39458286 Free PMC article. Review.
References
-
- Metlay JP, Waterer GW, Long AC, Anzueto A, Brozek J, Crothers K, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi: 10.1164/rccm.201908-1581ST. - DOI - PMC - PubMed
-
- Osman M, Manosuthi W, Kaewkungwal J, Silachamroon U, Mansanguan C, Kamolratanakul S, et al. Etiology, clinical course, and outcomes of pneumonia in the elderly: a retrospective and prospective cohort study in Thailand. Am J Trop Med Hyg. 2021;104(6):2009–2016. doi: 10.4269/ajtmh.20-1393. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
