

Lymphocyte recovery from radiation-induced lymphopenia in locally advanced esophageal squamous cell carcinoma: correlations with prognosis and lymphocyte-related organs
- PMID: 37858121
- PMCID: PMC10588237
- DOI: 10.1186/s13014-023-02354-w
Lymphocyte recovery from radiation-induced lymphopenia in locally advanced esophageal squamous cell carcinoma: correlations with prognosis and lymphocyte-related organs
Abstract
Background: Limited studies explored the relationship between lymphocyte recovery after definitive concurrent chemoradiotherapy (dCCRT) and prognosis in esophageal squamous cell carcinoma (ESCC).
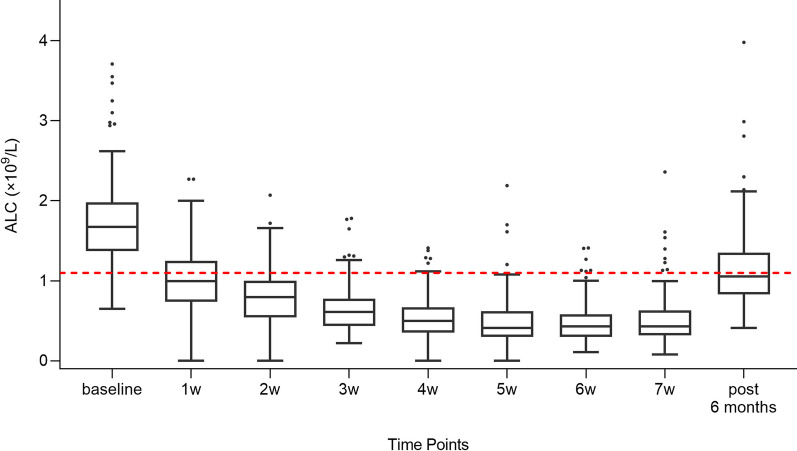
Methods: ESCC patients with obtainable absolute lymphocyte counts (ALCs) at 6 months after dCCRT were screened from prospective trials. Patients were divided into groups according to the grade of ALC nadir during radiotherapy (G4 or G1-3) and lymphocyte recovery status, which was assessed by lymphocyte recovery index (LRI), calculated as the ratio of post- to pre-treatment lymphocyte counts. Cox analysis was conducted to evaluate the prognostic significance of lymphocyte recovery status. Irradiated relative volumes of the bone marrow (BM) and spleen and effective dose to immune cells (EDIC) were collected to identify their impacts on lymphocyte recovery status by logistic analysis.
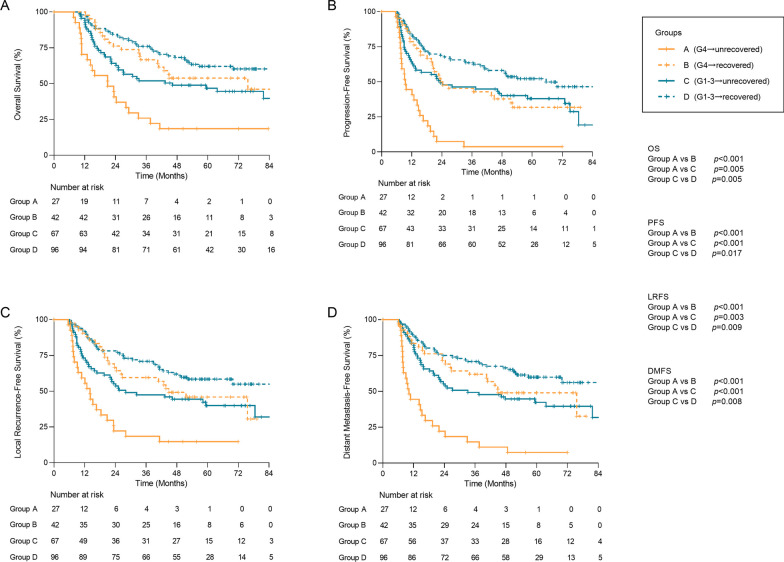
Results: 232 patients were enrolled. In 69 patients with G4 ALC nadir (group A and B) and 163 patients with G1-3 ALC nadir (group C and D) during dCCRT, 27 (group A) and 67 (group C) patients showed an insufficient level of lymphocyte recovery (LRI < 60%), and 42 (group B) and 96 (group D) patients showed a satisfactory level of lymphocyte recovery (LRI ≥ 60%). Cox multivariable analysis revealed that inadequate lymphocyte recovery was significantly associated with worse overall survival (HR, 2.80 and 1.70) and local recurrence-free survival (HR, 2.82 and 1.60) both in group A vs group B and group C vs group D. Logistic analysis identified BM V5 (OR 4.24 and 2.29) as an independent predictor of inadequate lymphocyte recovery from G4 or G1-3 ALC nadir, respectively.
Conclusions: Insufficient lymphocyte recovery might serve as a valuable prognostic factor, regardless of whether patients experienced G4 or G1-3 ALC nadir during radiotherapy. Additionally, it was observed that a larger relative volume of BM receiving ≥ 5 Gy was correlated with a higher risk of insufficient lymphocyte recovery.
Keywords: Chemoradiotherapy; Esophageal cancer; Lymphocyte; Recovery.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
None declared.
Figures
References
-
- Heier HE, Christensen I, Froland SS, et al. Early and late effects of irradiation for seminoma testis on the number of blood lymphocytes and their B and T subpopulations. Lymphology. 1975;8(3):69. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
