

Impact of piperaquine resistance in Plasmodium falciparum on malaria treatment effectiveness in The Guianas: a descriptive epidemiological study
- PMID: 37858325
- PMCID: PMC10808503
- DOI: 10.1016/S1473-3099(23)00502-9
Impact of piperaquine resistance in Plasmodium falciparum on malaria treatment effectiveness in The Guianas: a descriptive epidemiological study
Erratum in
-
Correction to Lancet Infect Dis 2023; published online Oct 16. https://doi.org/10.1016/S1473-3099(23)00502-9.Lancet Infect Dis. 2024 Feb;24(2):e83. doi: 10.1016/S1473-3099(23)00814-9. Epub 2023 Dec 18. Lancet Infect Dis. 2024. PMID: 38128562 Free PMC article. No abstract available.
Abstract
Background: Plasmodium falciparum is an apicomplexan parasite responsible for lethal cases of malaria. According to WHO recommendations, P falciparum cases are treated with artemisinin-based combination therapy including dihydroartemisinin-piperaquine. However, the emergence of resistant parasites against dihydroartemisinin-piperaquine was reported in southeast Asia in 2008 and, a few years later, suspected in South America.
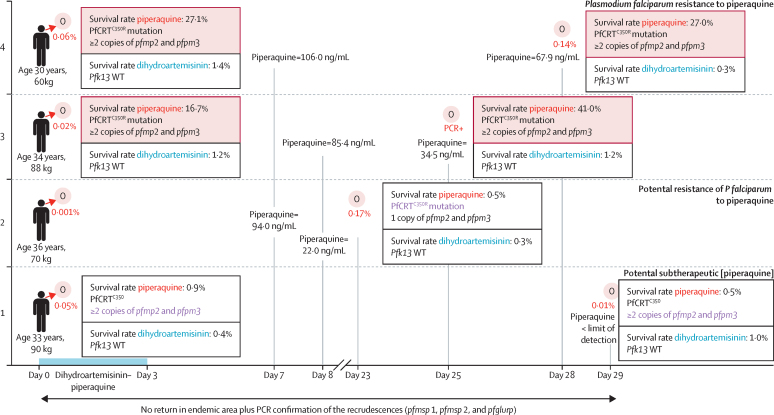
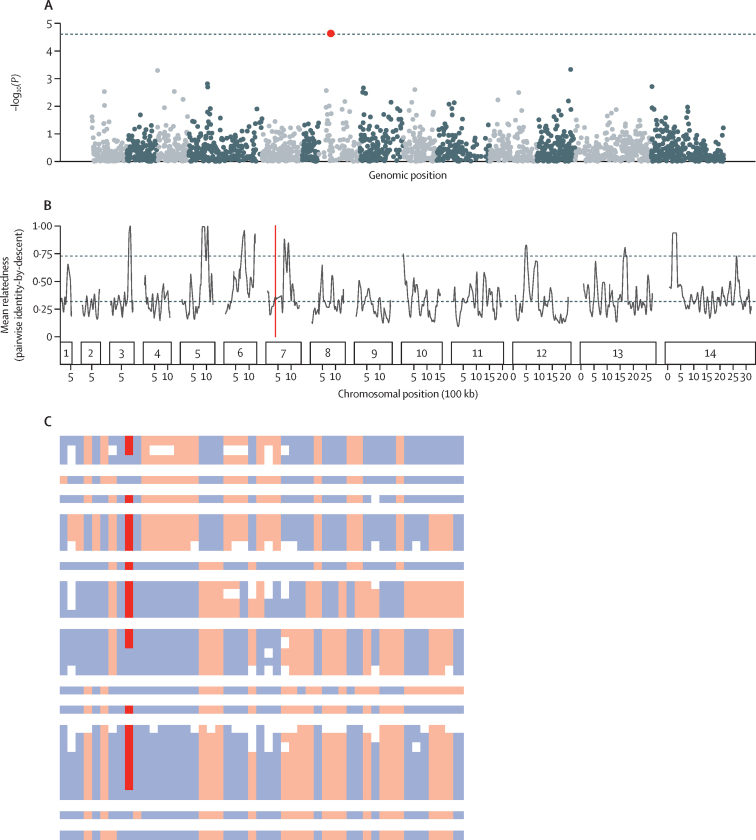
Methods: To characterise resistance emergence, a treatment efficacy study was performed on the reported patients infected with P falciparum and treated with dihydroartemisinin-piperaquine in French Guiana (n=6, 2016-18). Contemporary isolates collected in French Guiana were genotyped for P falciparum chloroquine resistance transporter (pfCRT; n=845) and pfpm2 and pfpm3 copy number (n=231), phenotyped using the in vitro piperaquine survival assay (n=86), and analysed through genomic studies (n=50). Additional samples from five Amazonian countries and one outside the region were genotyped (n=1440).
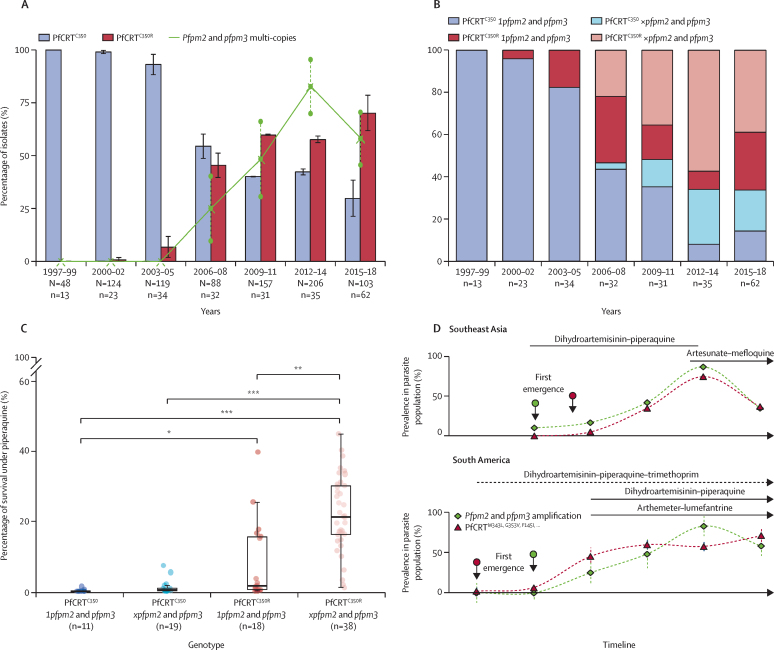
Findings: In field isolates, 40 (47%) of 86 (95% CI 35·9-57·1) were resistant to piperaquine in vitro; these phenotypes were more associated with pfCRTC350R (ie, Cys350Arg) and pfpm2 and pfpm3 amplifications (Dunn test, p<0·001). Those markers were also associated with dihydroartemisinin-piperaquine treatment failure (n=3 [50%] of 6). A high prevalence of piperaquine resistance markers was observed in Suriname in 19 (83%) of 35 isolates and in Guyana in 579 (73%) of 791 isolates. The pfCRTC350R mutation emerged before pfpm2 and pfpm3 amplification in a temporal sequence different from southeast Asia, and in the absence of artemisinin partial resistance, suggesting a geographically distinctive epistatic relationship between these genetic markers.
Interpretation: The high prevalence of piperaquine resistance markers in parasite populations of the Guianas, and the risk of associated therapeutic failures calls for caution on dihydroartemisinin-piperaquine use in the region. Furthermore, greater attention should be given to potential differences in genotype to phenotype mapping across genetically distinct parasite populations from different continents.
Funding: Pan American Health Organization and WHO, French Ministry for Research, European Commission, Santé publique France, Agence Nationale de la Recherche, Fundação de Amparo à Pesquisa do Estado do Amazonas, Ministry of Health of Brazil, Oswaldo Cruz Foundation, and National Institutes of Health.
Translations: For the French and Portuguese translations of the abstract see Supplementary Materials section.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests M-PA and PR are staff members of WHO. The authors alone are responsible for the views expressed in this publication, which do not necessarily represent the decisions, policies, or views of WHO. All other authors declare no competing interests.
Figures


References
-
- WHO . World Health Organization Press; Geneva: 2022. World malaria report 2022.
-
- Saunders DL, Vanachayangkul P, Lon C, et al. Dihydroartemisinin-piperaquine failure in Cambodia. N Engl J Med. 2014;371:484–485. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
