

Use and accuracy of decision support systems using artificial intelligence for tumor diseases: a systematic review and meta-analysis
- PMID: 37860189
- PMCID: PMC10584147
- DOI: 10.3389/fonc.2023.1224347
Use and accuracy of decision support systems using artificial intelligence for tumor diseases: a systematic review and meta-analysis
Abstract
Background: For therapy planning in cancer patients multidisciplinary team meetings (MDM) are mandatory. Due to the high number of cases being discussed and significant workload of clinicians, Clinical Decision Support System (CDSS) may improve the clinical workflow.
Methods: This review and meta-analysis aims to provide an overview of the systems utilized and evaluate the correlation between a CDSS and MDM.
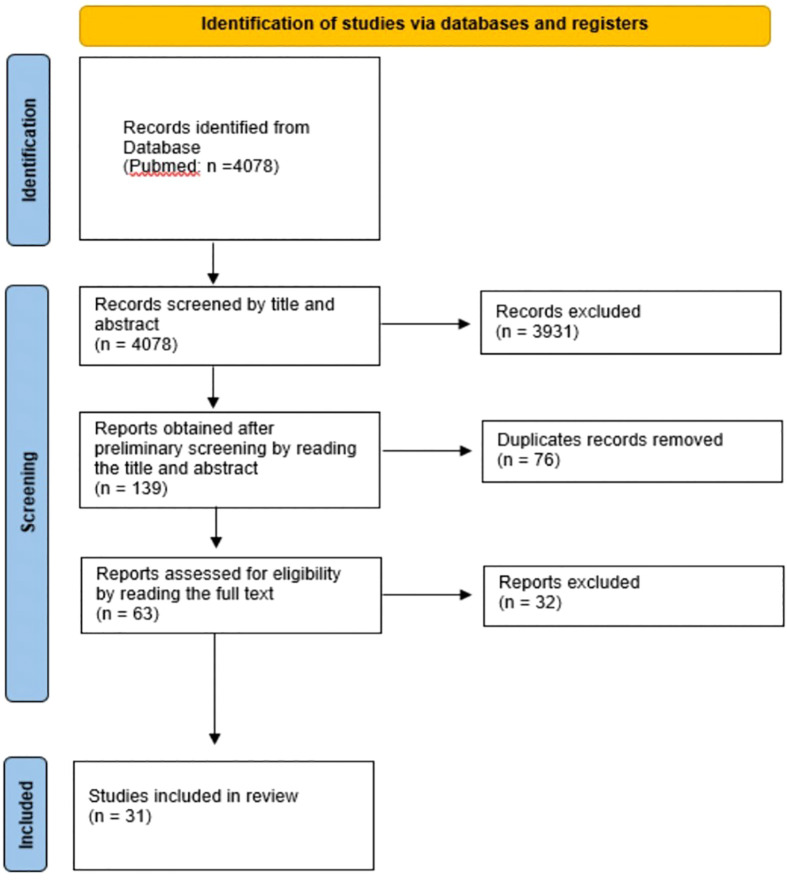
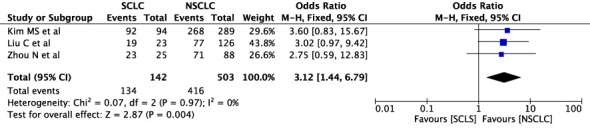
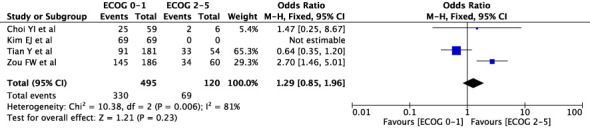
Results: A total of 31 studies were identified for final analysis. Analysis of different cancers shows a concordance rate (CR) of 72.7% for stage I-II and 73.4% for III-IV. For breast carcinoma, CR for stage I-II was 72.8% and for III-IV 84.1%, P≤ 0.00001. CR for colorectal carcinoma is 63% for stage I-II and 67% for III-IV, for gastric carcinoma 55% and 45%, and for lung carcinoma 85% and 83% respectively, all P>0.05. Analysis of SCLC and NSCLC yields a CR of 94,3% and 82,7%, P=0.004 and for adenocarcinoma and squamous cell carcinoma in lung cancer a CR of 90% and 86%, P=0.02.
Conclusion: CDSS has already been implemented in clinical practice, and while the findings suggest that its use is feasible for some cancers, further research is needed to fully evaluate its effectiveness.
Keywords: artificial intelligence; clinical decision support system; concordance between CDSS and MDS; machine learning; multidisciplinary team meetings.
Copyright © 2023 Oehring, Ramasetti, Ng, Roller, Thomas, Winter, Maurer, Moosburner, Raschzok, Kamali, Pratschke, Benzing and Krenzien.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous