

The incidence and risk factors of selected drug prescriptions and outpatient care after SARS-CoV-2 infection in low-risk subjects: a multicenter population-based cohort study
- PMID: 37860802
- PMCID: PMC10582710
- DOI: 10.3389/fpubh.2023.1241401
The incidence and risk factors of selected drug prescriptions and outpatient care after SARS-CoV-2 infection in low-risk subjects: a multicenter population-based cohort study
Abstract
Background: Knowledge about the dynamics of transmission of SARS-CoV-2 and the clinical aspects of COVID-19 has steadily increased over time, although evidence of the determinants of disease severity and duration is still limited and mainly focused on older adult and fragile populations.
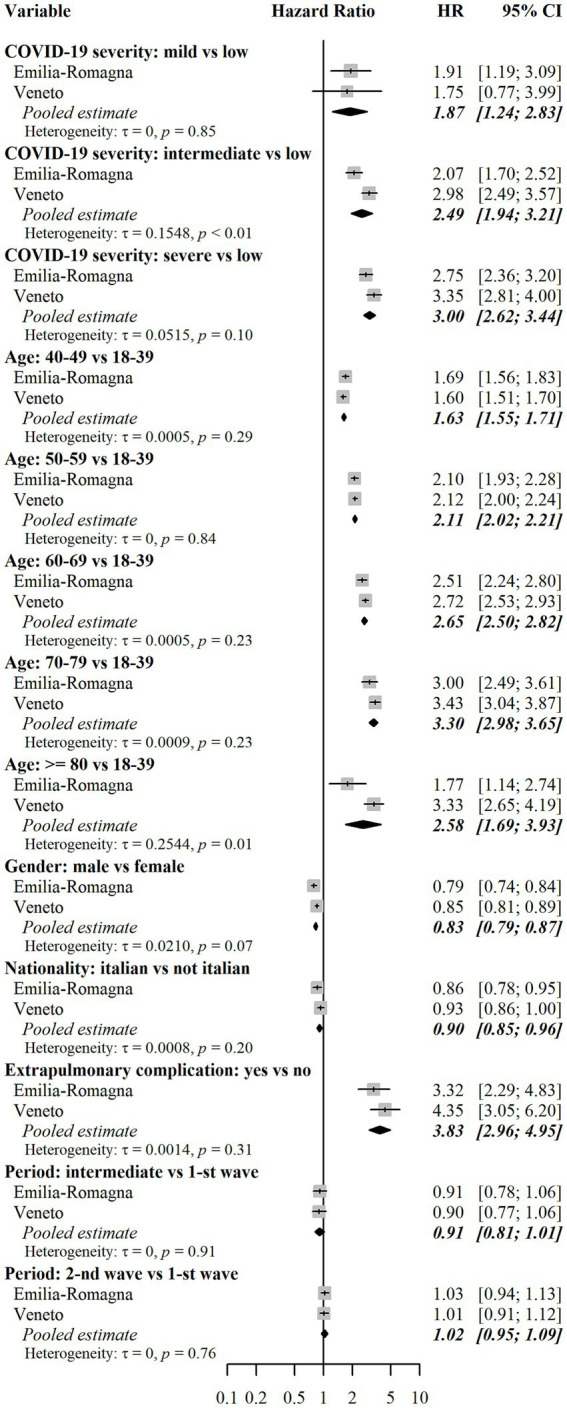
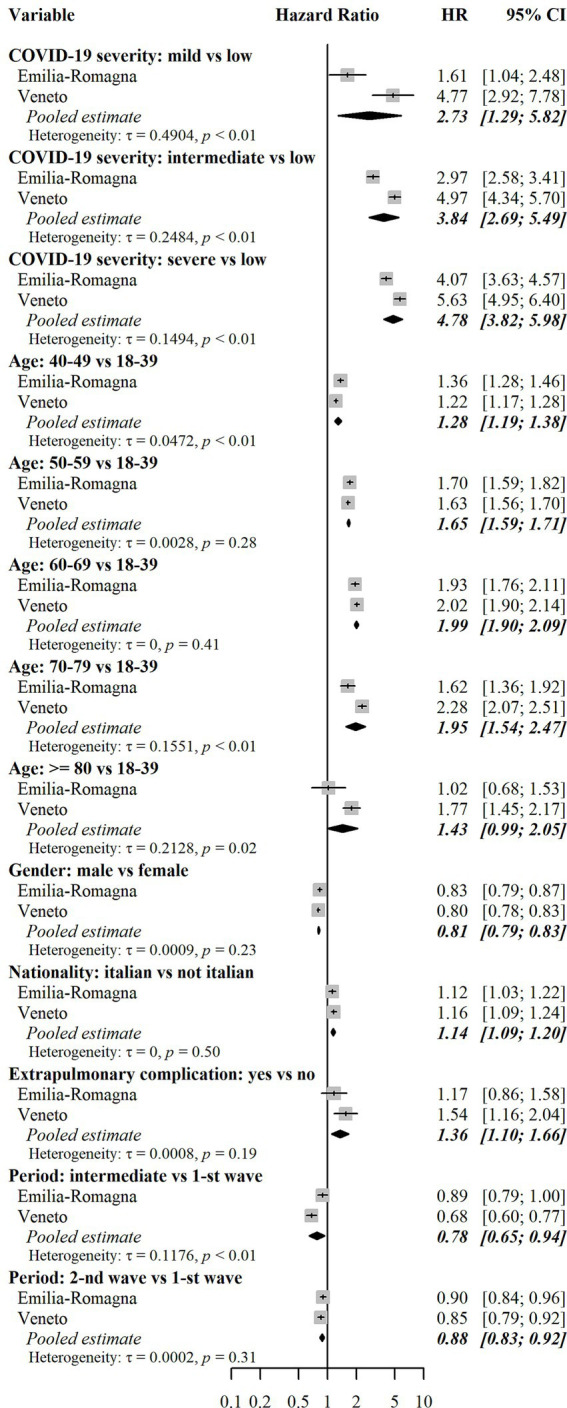
Methods: The present study was conceived and carried out in the Emilia-Romagna (E-R) and Veneto Regions, Italy, within the context of the EU's Horizon 2020 research project called ORCHESTRA (Connecting European Cohorts to increase common and effective response to SARS-CoV-2 pandemic) (www.orchestra-cohort.eu). The study has a multicenter retrospective population-based cohort design and aimed to investigate the incidence and risk factors of access to specific healthcare services (outpatient visits and diagnostics, drug prescriptions) during the post-acute phase from day-31 to day-365 after SARS-CoV-2 infection, in a healthy population at low risk of severe acute COVID-19. The study made use of previously recorded large-scale healthcare data available in the administrative databases of the two Italian Regions. The statistical analysis made use of methods for competing risks. Risk factors were assessed separately in the two Regions and results were pooled using random effects meta-analysis.
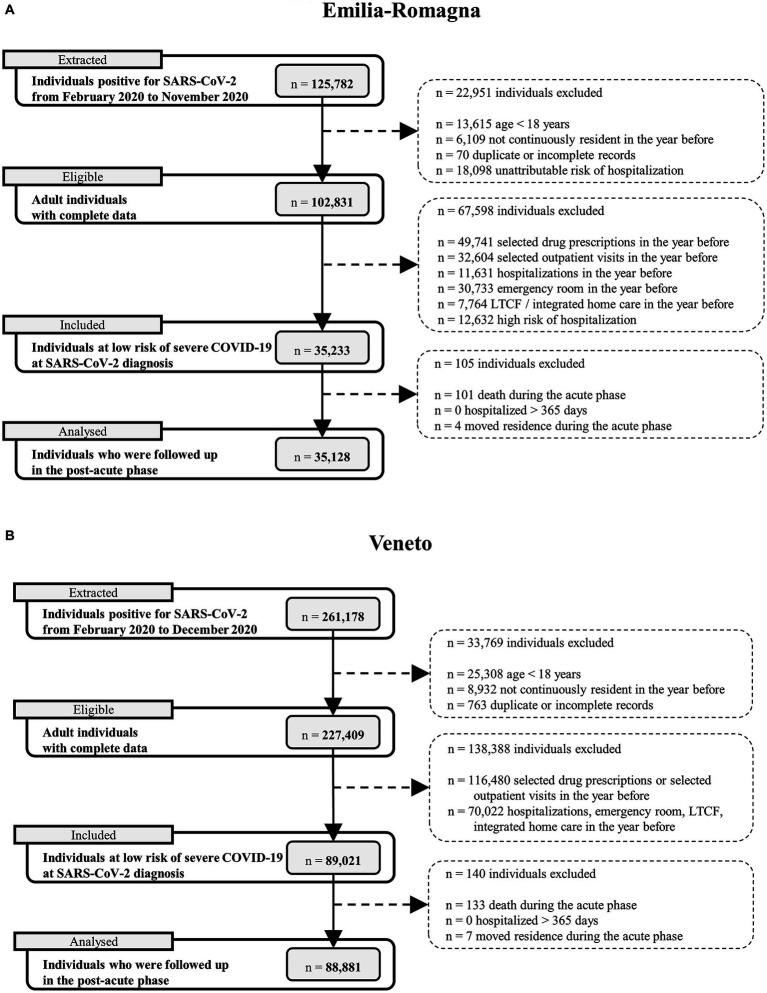
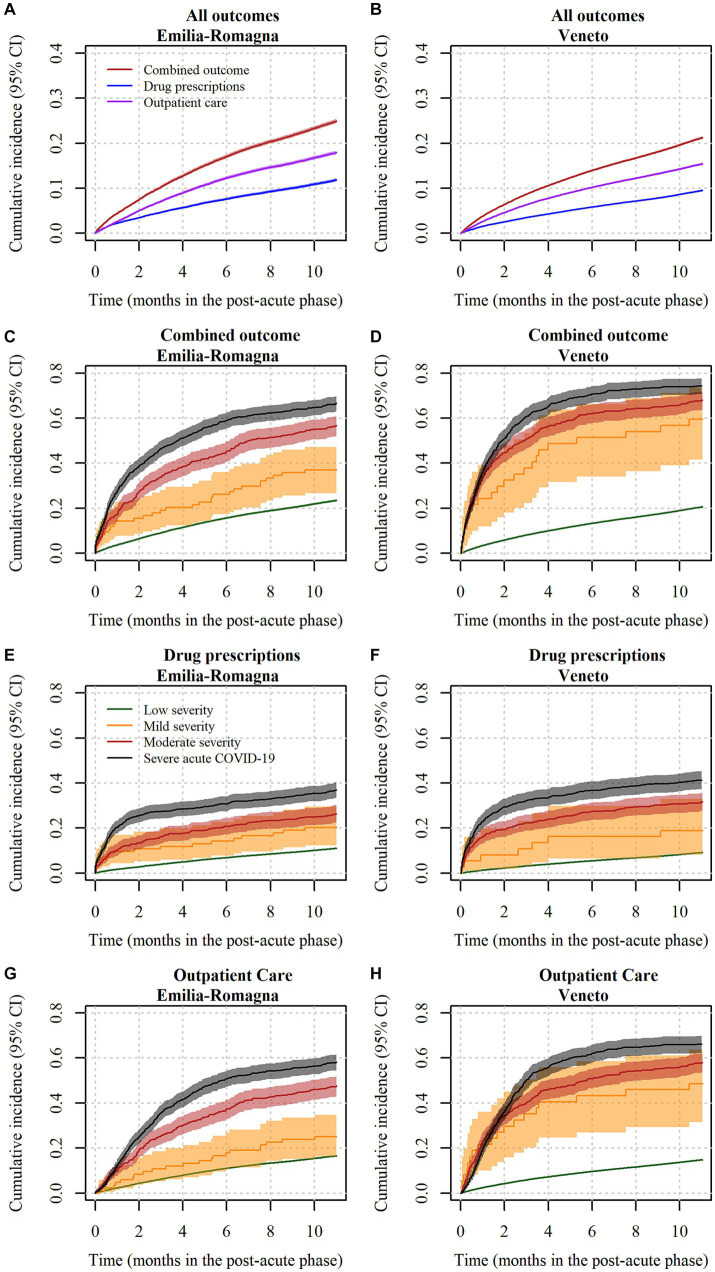
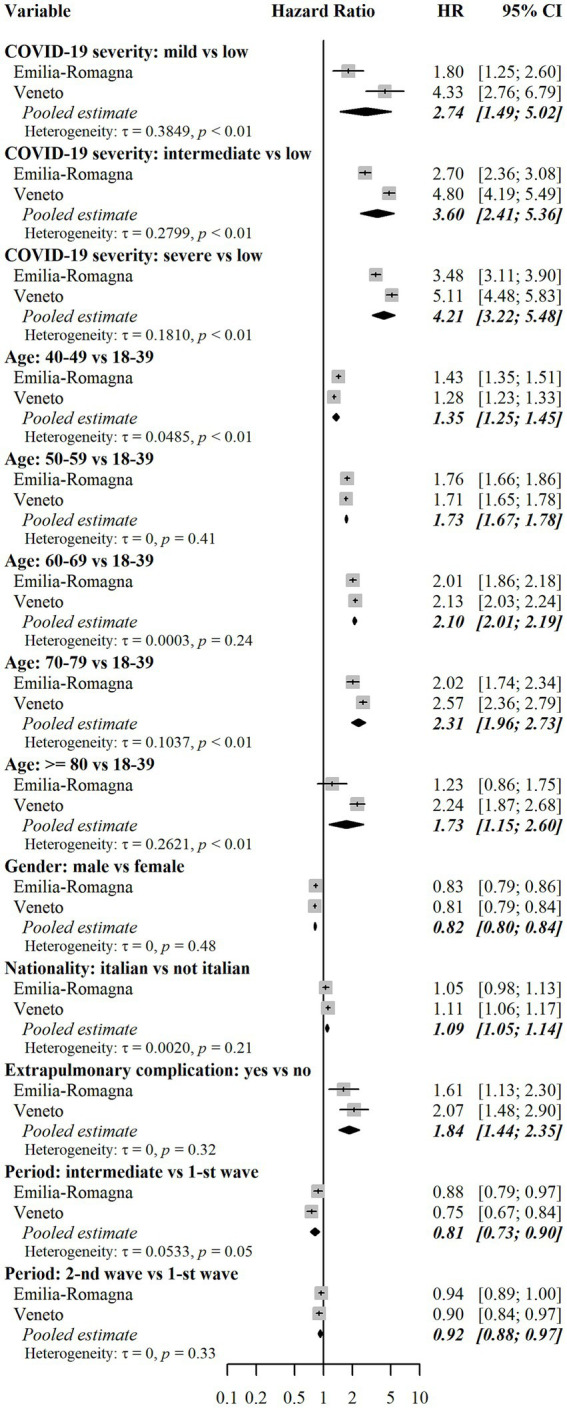
Results: There were 35,128 subjects in E-R and 88,881 in Veneto who were included in the data analysis. The outcome (access to selected health services) occurred in a high percentage of subjects in the post-acute phase (25% in E-R and 21% in Veneto). Outpatient care was observed more frequently than drug prescriptions (18% vs. 12% in E-R and 15% vs. 10% in Veneto). Risk factors associated with the outcome were female sex, age greater than 40 years, baseline risk of hospitalization and death, moderate to severe acute COVID-19, and acute extrapulmonary complications.
Conclusion: The outcome of interest may be considered as a proxy for long-term effects of COVID-19 needing clinical attention. Our data suggest that this outcome occurs in a substantial percentage of cases, even among a previously healthy population with low or mild severity of acute COVID-19. The study results provide useful insights into planning COVID-19-related services.
Keywords: COVID-19 sequelae; ORCHESTRA project; SARS-CoV-2; drug prescriptions; low-risk subjects; outpatient care; population-based cohort; post-COVID.
Copyright © 2023 Gagliotti, Banchelli, De Paoli, Buttazzi, Narne, Ricchizzi, Schievano, Bellio, Pitter, Tonon, Canziani, Rolli, Tacconelli, Berti, Russo and Moro.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Adeloye D, Elneima O, Daines L, Poinasamy K, Quint JK, Walker S, et al. The long-term sequelae of COVID-19: an international consensus on research priorities for patients with pre-existing and new-onset airways disease. Lancet Respir Med. (2021) 9:1467–78. doi: 10.1016/S2213-2600(21)00286-1, PMID: - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous