

An APRI+ALBI-Based Multivariable Model as a Preoperative Predictor for Posthepatectomy Liver Failure
- PMID: 37860868
- PMCID: PMC11974630
- DOI: 10.1097/SLA.0000000000006127
An APRI+ALBI-Based Multivariable Model as a Preoperative Predictor for Posthepatectomy Liver Failure
Abstract
Objective and background: Clinically significant posthepatectomy liver failure (PHLF B+C) remains the main cause of mortality after major hepatic resection. This study aimed to establish an aspartate aminotransferase to platelet ratio combined with an albumin-bilirubin grade (APRI+ALBI), based multivariable model (MVM) to predict PHLF and compare its performance to indocyanine green clearance (ICG-R15 or ICG-PDR) and albumin-ICG evaluation (ALICE).
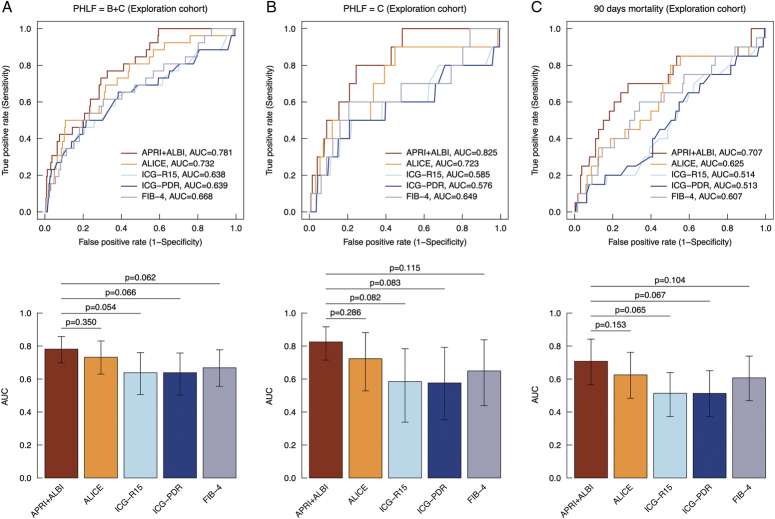
Methods: A total of 12,056 patients from the National Surgical Quality Improvement Program database were used to generate a MVM to predict PHLF B+C. The model was determined using stepwise backwards elimination. The performance of the model was tested using receiver operating characteristic curve analysis and validated in an international cohort of 2525 patients. In 620 patients, the APRI+ALBI MVM, trained in the National Surgical Quality Improvement Program cohort, was compared with the MVM's based on other liver function tests (ICG clearance, ALICE) by comparing the areas under the curve (AUC).
Results: A MVM including APRI+ALBI, age, sex, tumor type, and extent of resection was found to predict PHLF B+C with an AUC of 0.77, with comparable performance in the validation cohort (AUC: 0.74). In direct comparison with other MVM's based on more expensive and time-consuming liver function tests (ICG clearance, ALICE), the APRI+ALBI MVM demonstrated equal predictive potential for PHLF B+C. A smartphone application for the calculation of the APRI+ALBI MVM was designed.
Conclusion: Risk assessment through the APRI+ALBI MVM for PHLF B+C increases preoperative predictive accuracy and represents a universally available and cost-effective risk assessment before hepatectomy, facilitated by a freely available smartphone app.
Keywords: 90-day mortality; ALICE grade; APRI+ALBI; ICG clearance; liver surgery.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
P.S. and J.S. were involved in the development of a freely available smartphone-first application (TELLAPRIALBI, https://tellaprialbi.howto.health ). The remaining authors report no conflicts of interest.
Figures



Comment in
-
Risk predictors of post-hepatectomy liver failure: unraveling complexities and navigating challenges in clinical application.Hepatobiliary Surg Nutr. 2024 Jun 1;13(3):500-504. doi: 10.21037/hbsn-24-81. Epub 2024 May 24. Hepatobiliary Surg Nutr. 2024. PMID: 38911195 Free PMC article. No abstract available.
-
Non-invasive strategies to predict post-hepatectomy liver failure.Hepatobiliary Surg Nutr. 2024 Jun 1;13(3):533-535. doi: 10.21037/hbsn-24-219. Epub 2024 May 24. Hepatobiliary Surg Nutr. 2024. PMID: 38911211 Free PMC article. No abstract available.
References
-
- Gilg S, Sandström P, Rizell M, et al. . The impact of post-hepatectomy liver failure on mortality: a population-based study. Scand J Gastroenterol. 2018;53:1335–1339. - PubMed
-
- Gruenberger T, Bridgewater J, Chau I, et al. . Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: the OLIVIA multinational randomised phase II trial. Ann Oncol. 2015;26:702–708. - PubMed
-
- Nordlinger B, Sorbye H, Glimelius B, et al. . Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013;14:1208–1215. - PubMed
-
- Zorzi D, Laurent A, Pawlik TM, et al. . Chemotherapy-associated hepatotoxicity and surgery for colorectal liver metastases. Br J Surg. 2007;94:274–286. - PubMed
