

Phase I Dose-Escalation Study of the Safety and Pharmacokinetics of AGS15E Monotherapy in Patients with Metastatic Urothelial Carcinoma
- PMID: 37861407
- PMCID: PMC10767306
- DOI: 10.1158/1078-0432.CCR-22-3627
Phase I Dose-Escalation Study of the Safety and Pharmacokinetics of AGS15E Monotherapy in Patients with Metastatic Urothelial Carcinoma
Abstract
Purpose: Effective treatment of locally advanced or metastatic urothelial carcinoma (mUC) remains an unmet need. Antibody-drug conjugates (ADC) providing targeted drug delivery have shown antitumor activity in this setting. AGS15E is an investigational ADC that delivers the cytotoxic drug monomethyl auristatin E to cells expressing SLITRK6, a UC-associated antigen.
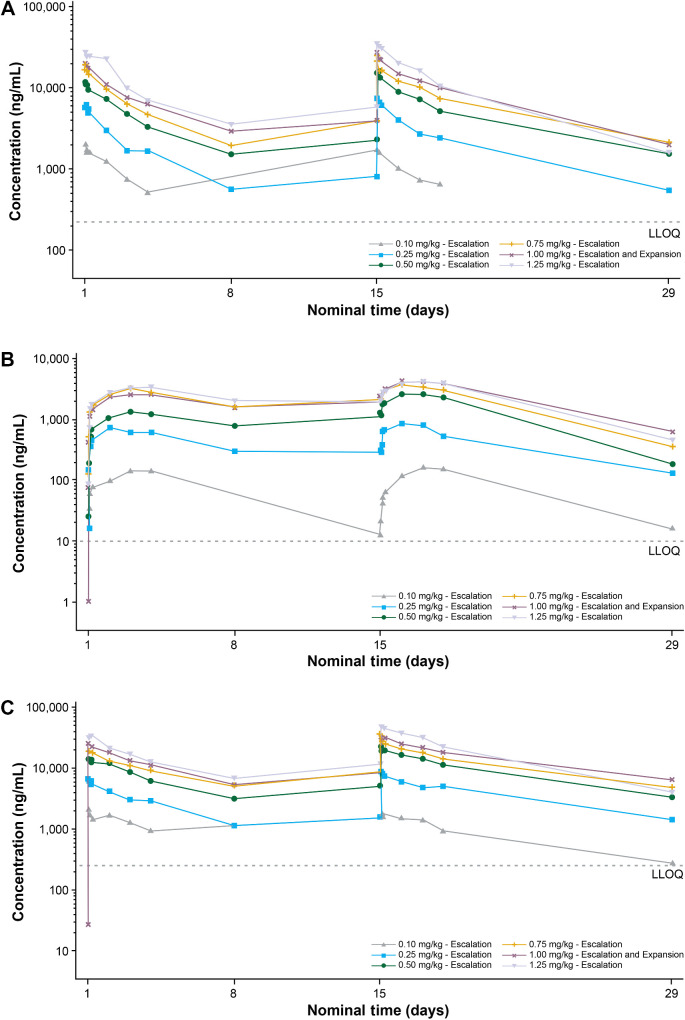
Patients and methods: This was a multicenter, single-arm, phase I dose-escalation and expansion trial of AGS15E in patients with mUC (NCT01963052). During dose escalation, AGS15E was administered intravenously at six levels (0.10, 0.25, 0.50, 0.75, 1.00, 1.25 mg/kg), employing a continual reassessment method to determine dose-limiting toxicities (DLT) and the recommended phase II dose (RP2D) for the dose-expansion cohort. The primary objective was to evaluate the safety and pharmacokinetics of AGS15E in patients with and without prior chemotherapy and with prior checkpoint inhibitor (CPI) therapy. Best overall response was also examined.
Results: Ninety-three patients were recruited, including 33 patients previously treated with CPI. The most common treatment-emergent adverse events were fatigue (54.8%), nausea (37.6%), and decreased appetite (35.5%). Peripheral neuropathy and ocular toxicities occurred at doses of ≥0.75 mg/kg. AGS15E increased in a dose-proportional manner after single- and multiple-dose administration; accumulation was low. Five DLT occurred from 0.50 to 1.25 mg/kg. The RP2D was assessed at 1.00 mg/kg; the objective response rate (ORR) was 35.7% at this dose level. The ORR in the total population and CPI-exposed subgroup were 18.3% and 27.3%, respectively.
Conclusions: DLT with AGS15E were observed at 0.75, 1.00, and 1.25 mg/kg, with an RP2D of 1.00 mg/kg being determined.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures


References
-
- Bellmunt J, Valderrama BP, Puente J, Grande E, Bolos MV, Lainez N, et al. Recent therapeutic advances in urothelial carcinoma: a paradigm shift in disease management. Crit Rev Oncol Hematol 2022;174:103683. - PubMed
-
- De Santis M, Bellmunt J, Mead G, Kerst JM, Leahy M, Maroto P, et al. Randomized phase II/III trial assessing gemcitabine/carboplatin and methotrexate/carboplatin/vinblastine in patients with advanced urothelial cancer who are unfit for cisplatin-based chemotherapy: EORTC study 30986. J Clin Oncol 2012;30:191–9. - PMC - PubMed
-
- Keytruda (pembrolizumab) [package insert]. Rahway, NJ: Merck Sharpe & Dohme; 2023.
-
- Padcev (enfortumab vedotin) [package insert]. Northbrook, IL: Astellas Pharma US, Inc. and Bothell, WA: Seagen Inc.; 2023.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
