

Association of urine biomarkers of kidney health with subclinical cardiovascular disease among men with and without HIV
- PMID: 37861689
- PMCID: PMC10922264
- DOI: 10.1097/QAD.0000000000003761
Association of urine biomarkers of kidney health with subclinical cardiovascular disease among men with and without HIV
Abstract
Objective: The aim of this study was to determine whether urine biomarkers of kidney health are associated with subclinical cardiovascular disease among men with and without HIV.
Design: A cross-sectional study within the Multicenter AIDS Cohort Study (MACS) among 504 men with and without HIV infection who underwent cardiac computed tomography scans and had urine biomarkers measured within the preceding 2 years.
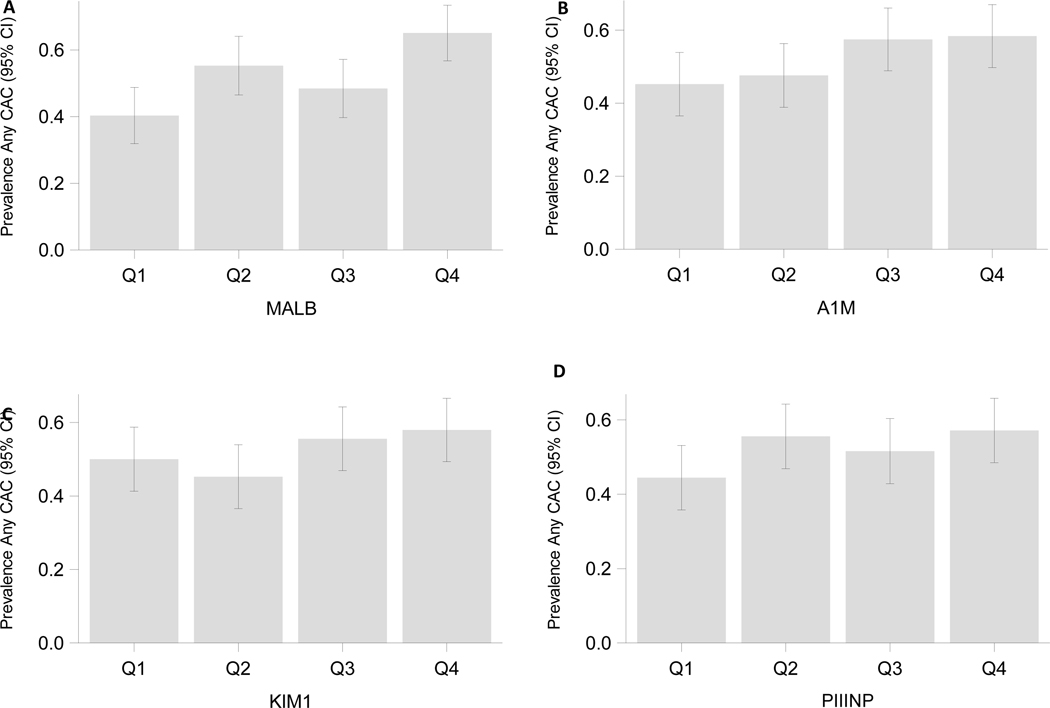
Methods: Our primary predictors were four urine biomarkers of endothelial (albuminuria), proximal tubule dysfunction (alpha-1-microglobulin [A1 M] and injury (kidney injury molecule-1 [KIM-1]) and tubulointerstitial fibrosis (pro-collagen-III N-terminal peptide [PIIINP]). These were evaluated for association with coronary artery calcium (CAC) prevalence, CAC extent, total plaque score, and total segment stenosis using multivariable regression.
Results: Of the 504 participants, 384 were men with HIV (MWH) and 120 were men without HIV. In models adjusted for sociodemographic factors, cardiovascular disease risk factors, eGFR, and HIV-related factors, each two-fold higher concentration of albuminuria was associated with a greater extent of CAC (1.35-fold higher, 95% confidence interval 1.11-1.65), and segment stenosis (1.08-fold greater, 95% confidence interval 1.01-1.16). Associations were similar between MWH and men without HIV in stratified analyses. The third quartile of A1 M showed an association with greater CAC extent, total plaque score, and total segment stenosis, compared with the lowest quartile.
Conclusion: Worse endothelial and proximal tubule dysfunction, as reflected by higher urine albumin and A1 M, were associated with greater CAC extent and coronary artery stenosis.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Figures


Comment in
-
A new frontier in HIV care: the predictive power of renal biomarkers on heart health.AIDS. 2024 Mar 15;38(4):595-596. doi: 10.1097/QAD.0000000000003819. Epub 2024 Feb 29. AIDS. 2024. PMID: 38416550 No abstract available.
References
-
- Senoner T, Barbieri F, Adukauskaite A, Sarcletti M, Plank F, Beyer C, et al. Coronary atherosclerosis characteristics in HIV-infected patients on long-term antiretroviral therapy: insights from coronary computed tomography–angiography: Erratum. AIDS 2020; 34(6):961–961. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL085757/HL/NHLBI NIH HHS/United States
- U01 DK114866/DK/NIDDK NIH HHS/United States
- U01 HL146245/HL/NHLBI NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- KL2 TR001432/TR/NCATS NIH HHS/United States
- U01 HL146192/HL/NHLBI NIH HHS/United States
- U01 HL146242/HL/NHLBI NIH HHS/United States
- TL1 TR001431/TR/NCATS NIH HHS/United States
- TL1 TR001871/TR/NCATS NIH HHS/United States
- R01 HL095129/HL/NHLBI NIH HHS/United States
- U01 HL146193/HL/NHLBI NIH HHS/United States
- U01 HL146194/HL/NHLBI NIH HHS/United States
- U01 HL146241/HL/NHLBI NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- U01 HL146333/HL/NHLBI NIH HHS/United States
- R01 DK093770/DK/NIDDK NIH HHS/United States
- U01 HL146205/HL/NHLBI NIH HHS/United States
- P30 DK079310/DK/NIDDK NIH HHS/United States
- P30 MH116867/MH/NIMH NIH HHS/United States
- U01 HL146208/HL/NHLBI NIH HHS/United States
- R01 AG034853/AG/NIA NIH HHS/United States
- U01 DK106962/DK/NIDDK NIH HHS/United States
- P30 AI073961/AI/NIAID NIH HHS/United States
- U01 HL146201/HL/NHLBI NIH HHS/United States
- U01 DK129984/DK/NIDDK NIH HHS/United States
- U01 HL146204/HL/NHLBI NIH HHS/United States
- U01 HL146202/HL/NHLBI NIH HHS/United States
- UL1 TR001881/TR/NCATS NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- U01 HL146240/HL/NHLBI NIH HHS/United States
- U01 HL146203/HL/NHLBI NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
