

Treatments and Severe Outcomes for Patients Diagnosed With MIS-C at Four Children's Hospitals in the United States, March 16, 2020-March 10, 2021
- PMID: 37862698
- PMCID: PMC11318085
- DOI: 10.1097/INF.0000000000004065
Treatments and Severe Outcomes for Patients Diagnosed With MIS-C at Four Children's Hospitals in the United States, March 16, 2020-March 10, 2021
Abstract
Background: Clinical management of multisystem inflammatory syndrome in children (MIS-C) has varied over time and by medical institution.
Methods: Data on patients with MIS-C were collected from 4 children's hospitals between March 16, 2020 and March 10, 2021. Relationships between MIS-C treatments and patient demographics, clinical characteristics, and outcomes were described. Propensity score matching was utilized to assess the relative risk of outcomes dependent on early treatment with intravenous immunoglobulin (IVIG) or low-dose steroids, controlling for potential confounding variables.
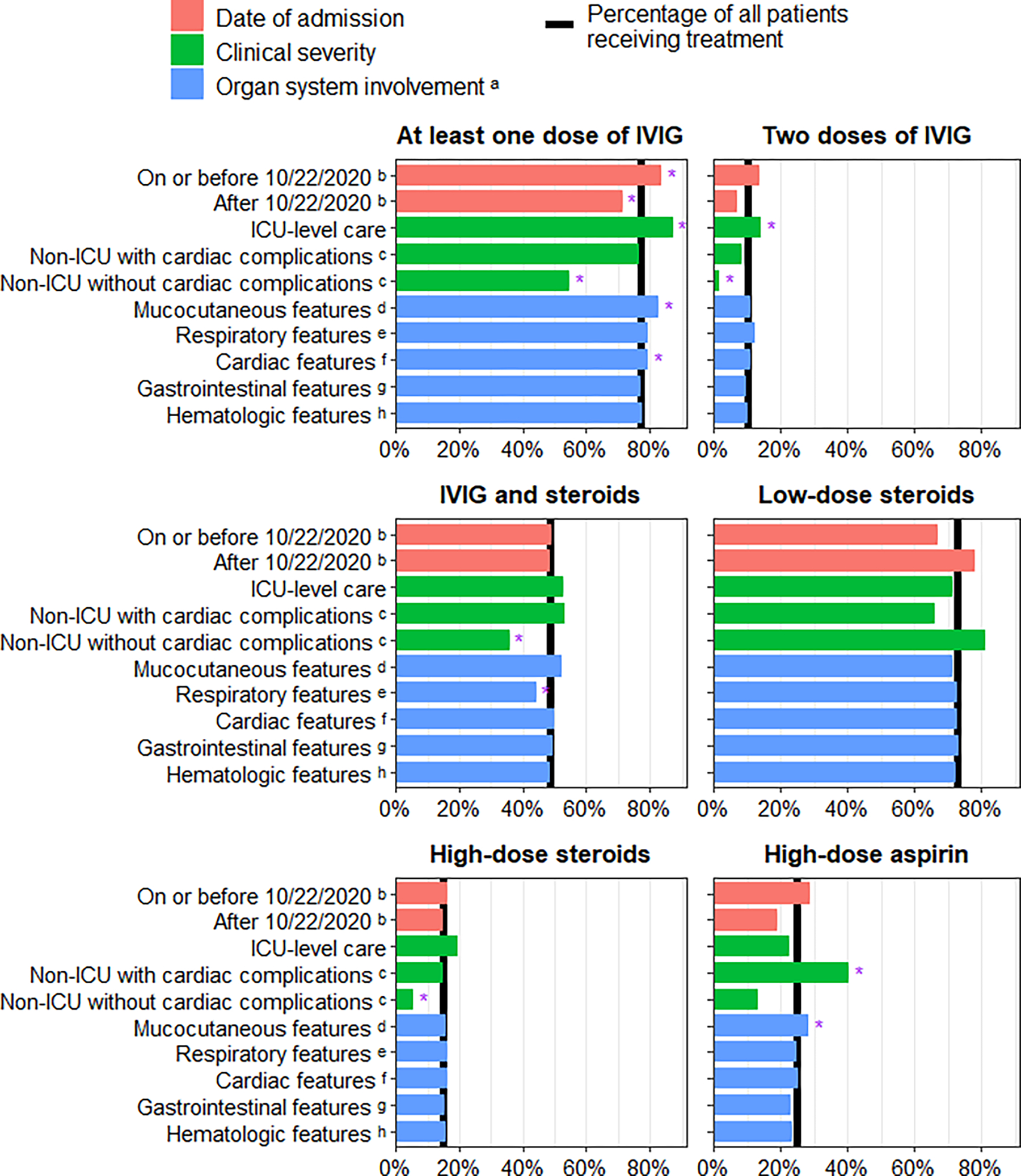
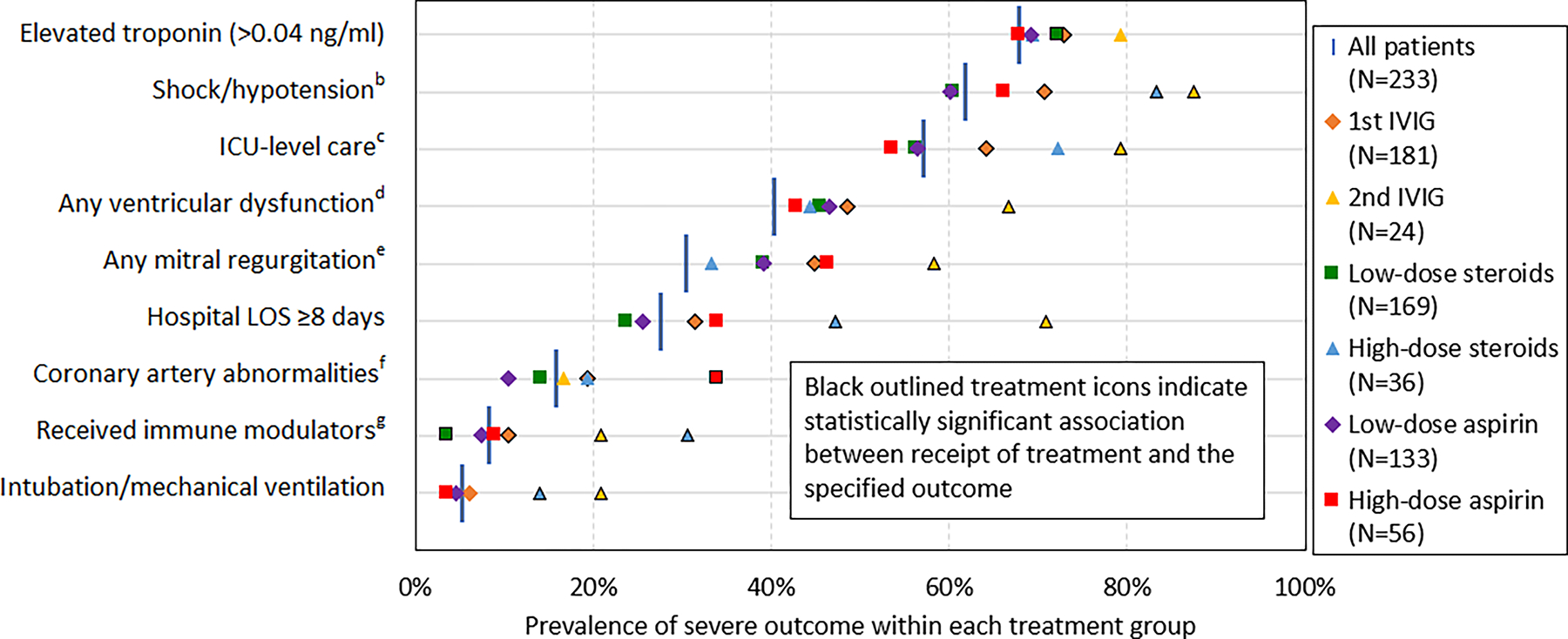
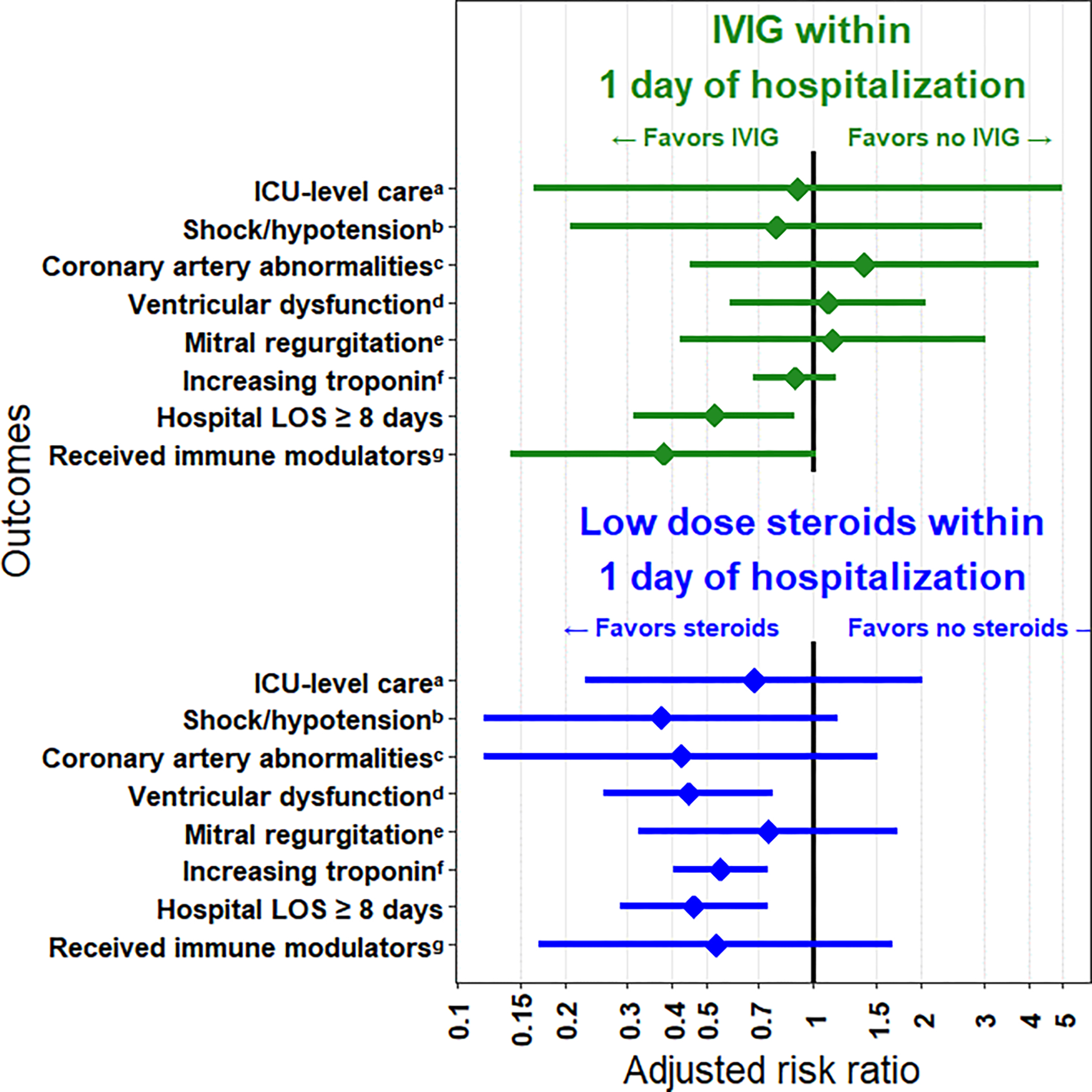
Results: Of 233 patients diagnosed with MIS-C, the most commonly administered treatments were steroids (88.4%), aspirin (81.1%), IVIG (77.7%) and anticoagulants (71.2%). Compared with those patients without respiratory features, patients with respiratory features were less likely to receive IVIG and steroids on the same day (combination treatment) (44.1%). Controlling for confounding variables, patients receiving IVIG within 1 day of hospitalization were less likely to have hospital length of stay ≥8 days (RR = 0.53, 95% CI: 0.31-0.88). Patients receiving low-dose steroids within 1 day of hospitalization were less likely to develop ventricular dysfunction (RR = 0.45, 95% CI: 0.26-0.77), have increasingly elevated troponin levels (RR = 0.55, 95% CI: 0.40-0.75) or have hospital length of stay ≥8 days (RR = 0.46, 95% CI: 0.29-0.74).
Conclusion: Treatments for MIS-C differed by hospital, patient characteristics and illness severity. When IVIG and low-dose steroids were administered in combination or low-dose steroids were administered alone within 1 day of hospitalization, the risk of subsequent severe outcomes was decreased.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
C.A.R.’s institution has received funds to conduct clinical research unrelated to this article from the National Institutes of Health, BioFire Inc, GSK, MedImmune, Micron, Janssen, Merck, Moderna, Novavax, PaxVax, Pfizer, Regeneron, Sanofi-Pasteur. She is a coinventor of patented respiratory syncytial virus (RSV) vaccine technology unrelated to this article, which has been licensed to Meissa Vaccines, Inc. Her institution has received funding from NIH to conduct clinical trials of Moderna and Janssen COVID-19 vaccines. M.E.O.’s institution has received funds from the National Institutes of Health for the evaluation of patients with MIS-C. C.M.K.’s institution has received funds from the National Institutes of Health to be a sub-site for the Moderna KIDCove COVID-19 vaccine clinical trial as part of Vaccine and Treatment Evaluations Unit network. All other authors have no conflicts of interest or funding to disclose.
Figures

References
-
- Morris SB, Schwartz NG, Patel P, Abbo L, Beauchamps L, Balan S, et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection - United Kingdom and United States, March-August 2020. MMWR Morb Mortal Wkly Rep. 2020. Oct 9;69(40):1450–6. doi: 10.15585/mmwr.mm6940e1. - DOI - PMC - PubMed
-
- Network CHA. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). CDC Health Alert Network; 2020.
-
- Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 2. Arthritis Rheumatol. 2021. Apr;73(4):e13–e29. doi: 10.1002/art.41616. - DOI - PMC - PubMed
-
- Pediatrics AAo. Multisystem Inflammatory Syndrome in Children (MIS-C) Interim Guidance. American Academy of Pediatrics; [updated August 25, 2022]; Available from: https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/....
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
