

Tumor-resident Lactobacillus iners confer chemoradiation resistance through lactate-induced metabolic rewiring
- PMID: 37863066
- PMCID: PMC10841640
- DOI: 10.1016/j.ccell.2023.09.012
Tumor-resident Lactobacillus iners confer chemoradiation resistance through lactate-induced metabolic rewiring
Abstract
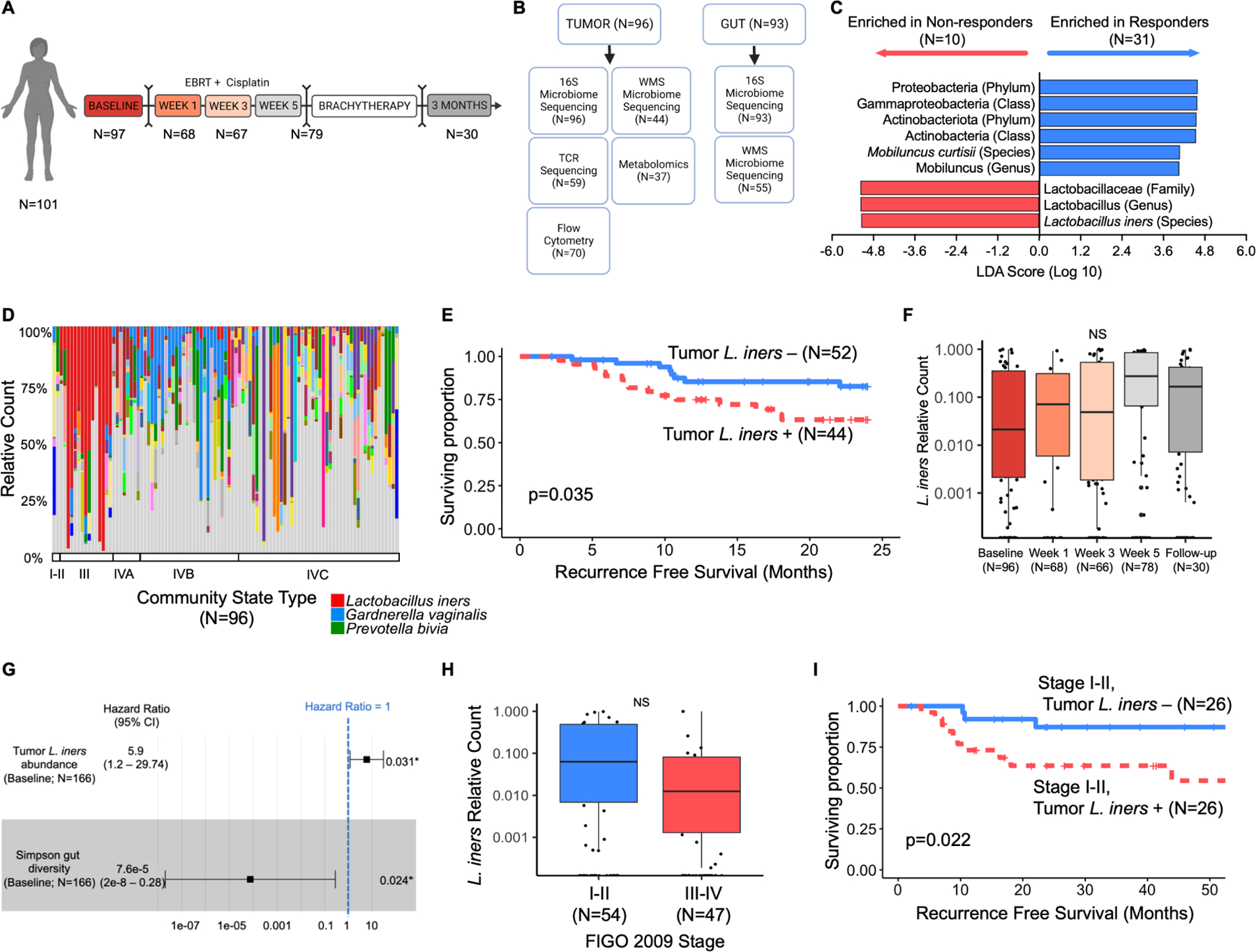
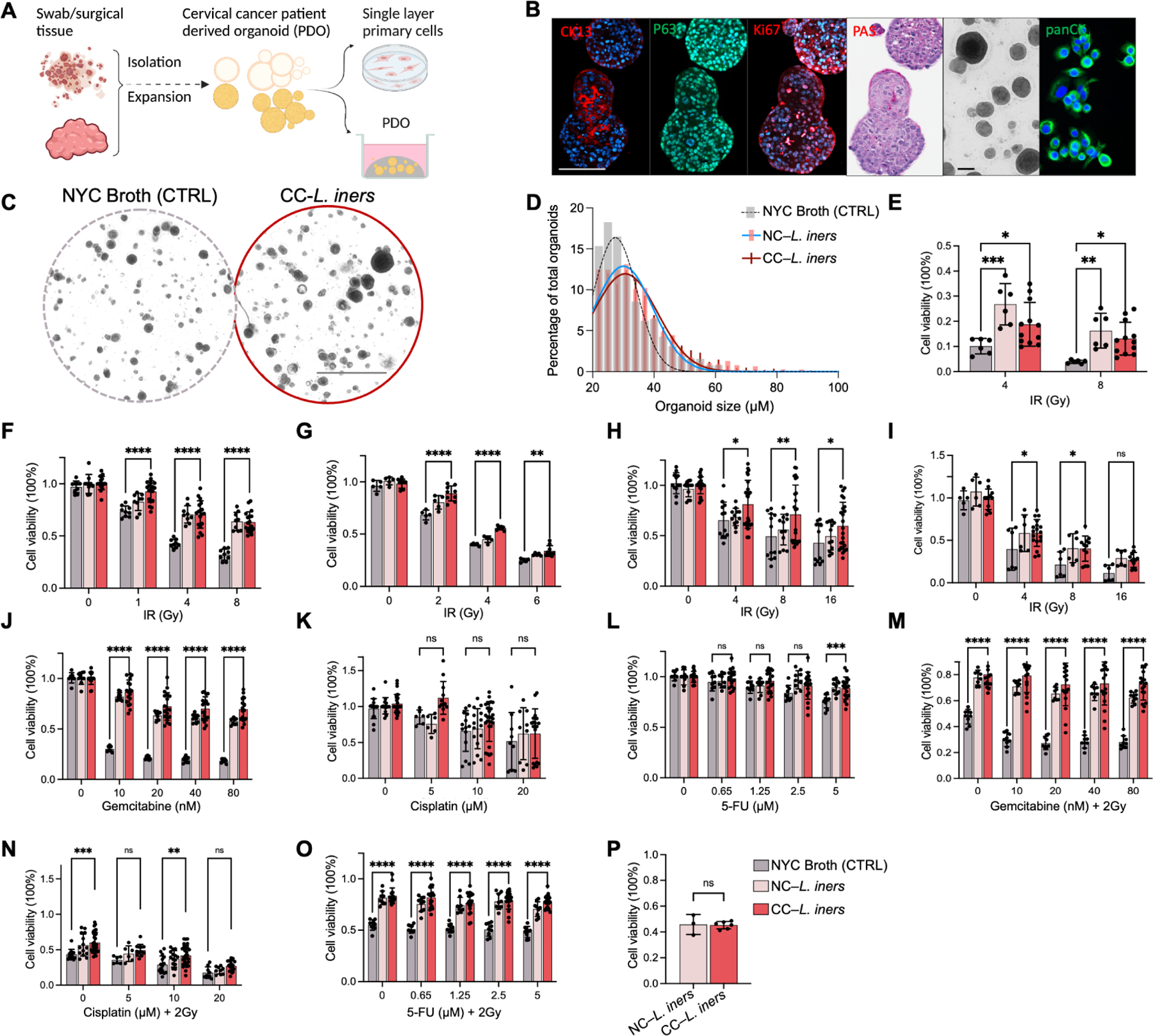
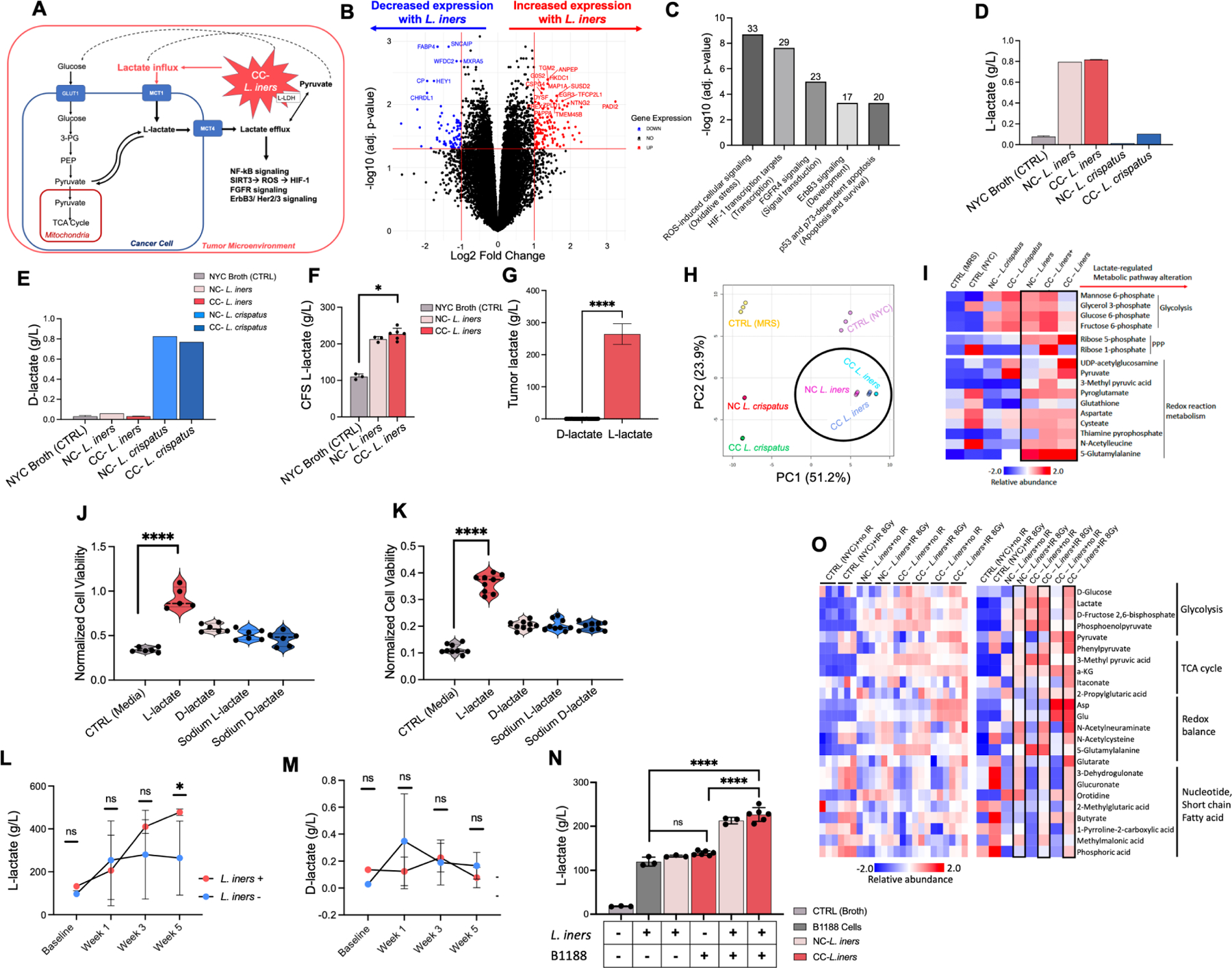
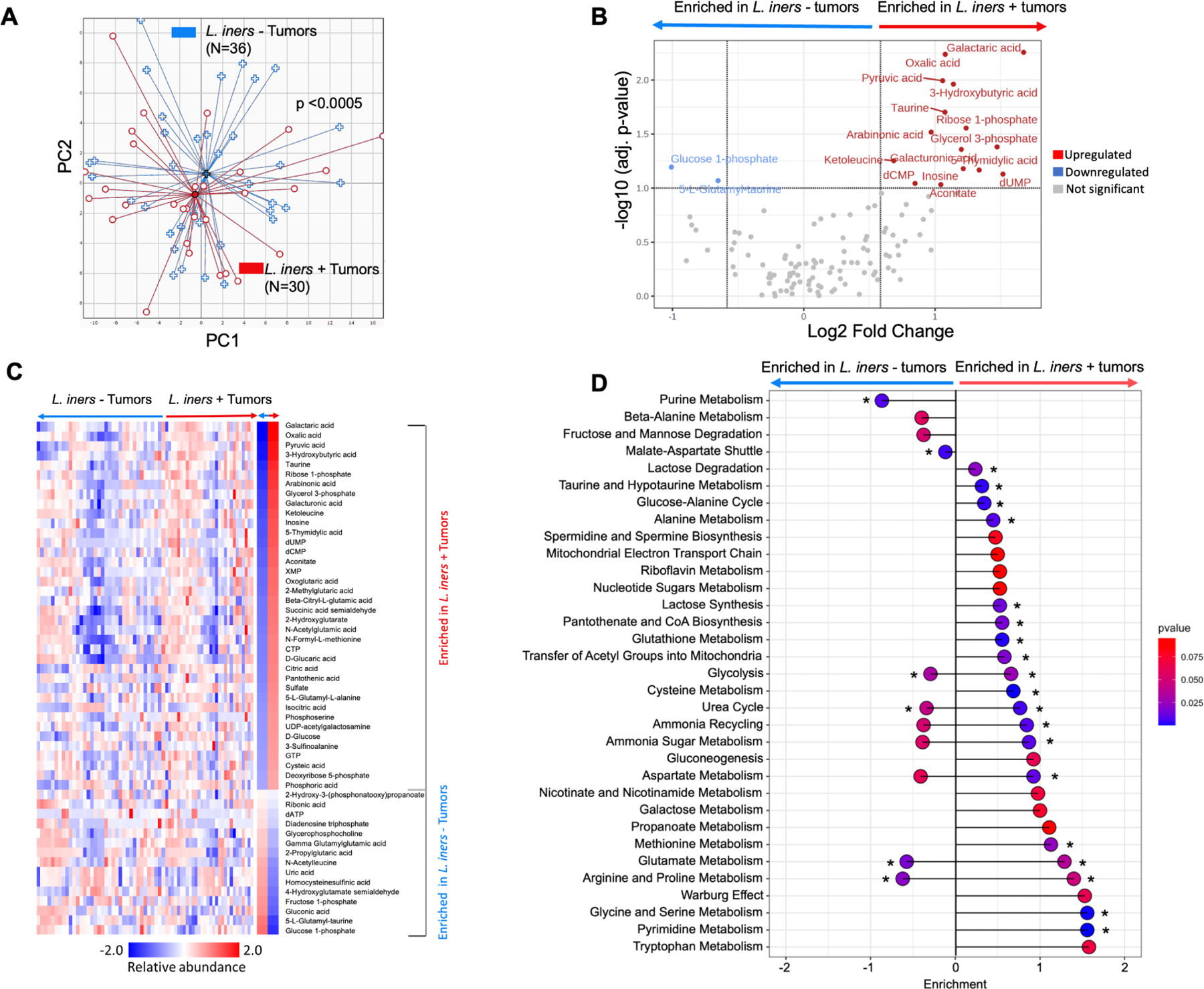
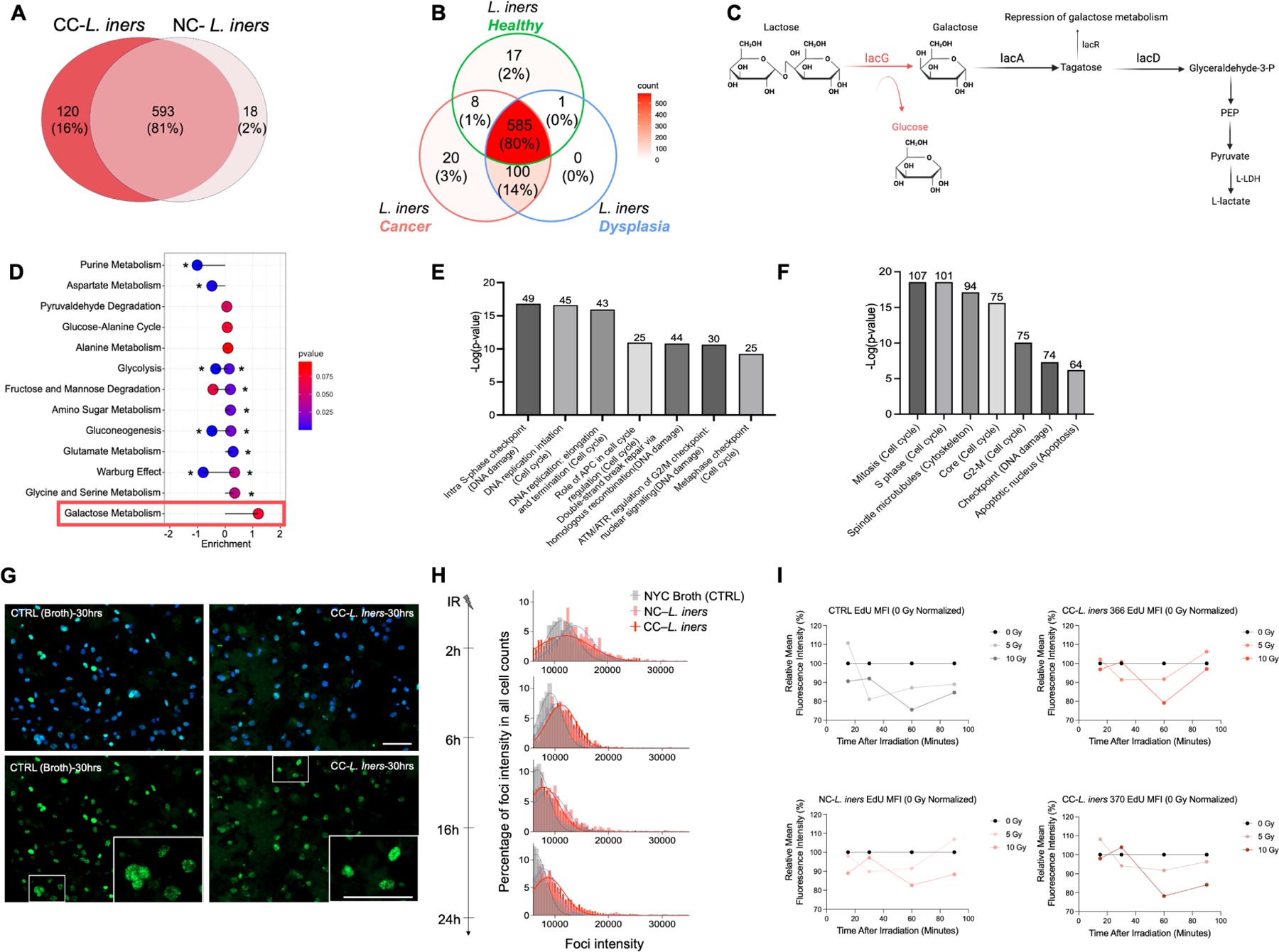
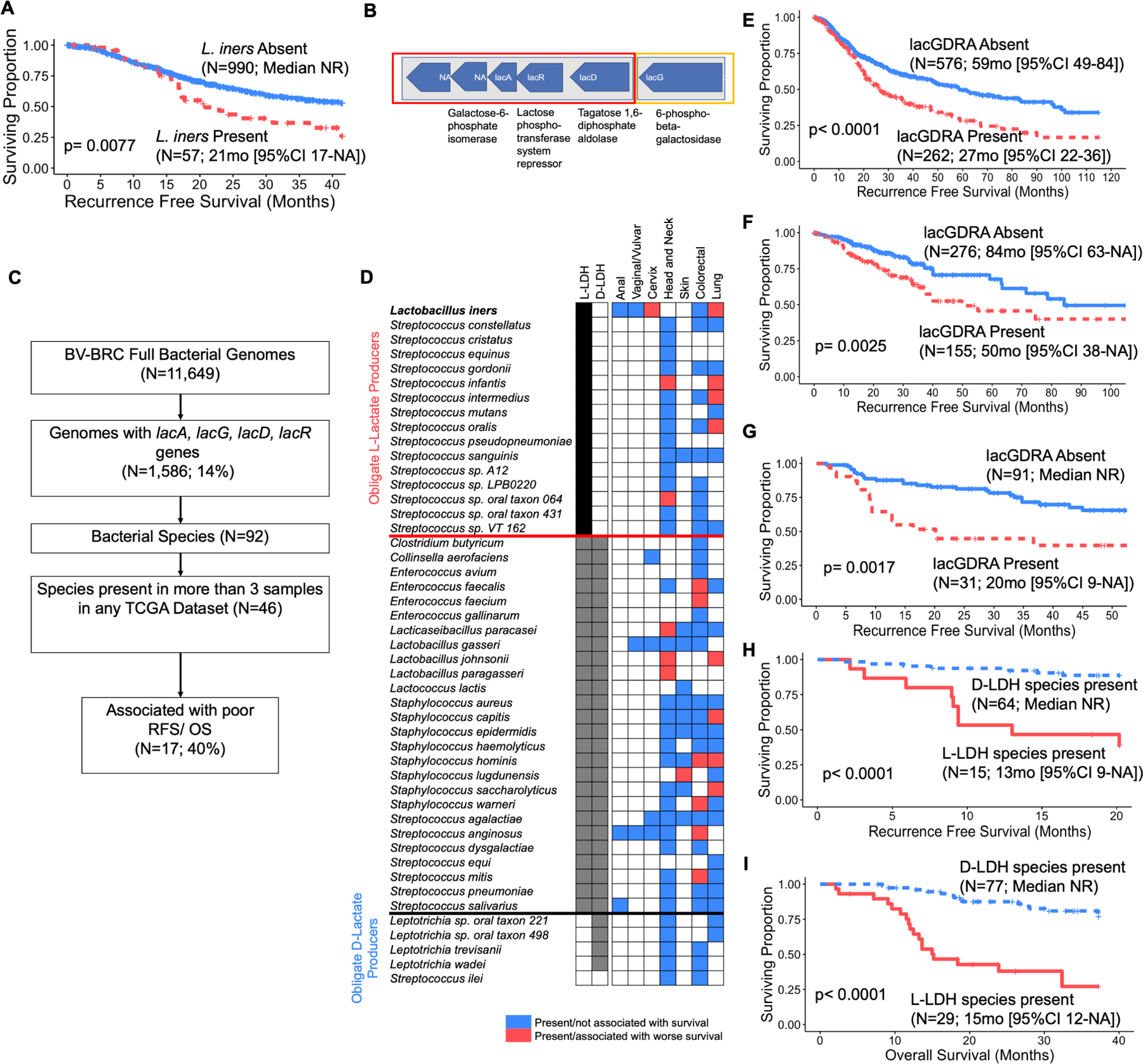
Tumor microbiota can produce active metabolites that affect cancer and immune cell signaling, metabolism, and proliferation. Here, we explore tumor and gut microbiome features that affect chemoradiation response in patients with cervical cancer using a combined approach of deep microbiome sequencing, targeted bacterial culture, and in vitro assays. We identify that an obligate L-lactate-producing lactic acid bacterium found in tumors, Lactobacillus iners, is associated with decreased survival in patients, induces chemotherapy and radiation resistance in cervical cancer cells, and leads to metabolic rewiring, or alterations in multiple metabolic pathways, in tumors. Genomically similar L-lactate-producing lactic acid bacteria commensal to other body sites are also significantly associated with survival in colorectal, lung, head and neck, and skin cancers. Our findings demonstrate that lactic acid bacteria in the tumor microenvironment can alter tumor metabolism and lactate signaling pathways, causing therapeutic resistance. Lactic acid bacteria could be promising therapeutic targets across cancer types.
Keywords: cervical cancer; chemoradiation; lactate; metabolism; microbiome; radiation.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests L.E.C. reports grants from American Society for Clinical Oncology, Radiology Society of North America, National Institutes of Health, and MD Anderson Cancer Center during the conduct of the study. A.J. reports personal fees from Genentech during the conduct of the study, as well as personal fees from Genentech outside the submitted work. L.L. reports other support from AstraZeneca and Pfizer, and grants from NCI outside the submitted work. J.A.W. reports other support from Micronoma during the conduct of the study, as well as other support from Imedex, Dava Oncology, Illumina, and PeerView outside the submitted work. P.O. reports Faculty grant/research support from Merck Sharp and Dohme Corp, Deinove Pharmaceuticals, Summit Pharmaceuticals, Melinta Pharmaceuticals, and Napo Pharmaceutical, in addition to consultant work with Napo Pharmaceutical, Ferring Pharmaceutical, Summit Pharmaceutical, and SNIPR Biome Company, all outside of the submitted work.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
