

Neoadjuvant camrelizumab plus nab-paclitaxel and epirubicin in early triple-negative breast cancer: a single-arm phase II trial
- PMID: 37863916
- PMCID: PMC10589334
- DOI: 10.1038/s41467-023-42479-w
Neoadjuvant camrelizumab plus nab-paclitaxel and epirubicin in early triple-negative breast cancer: a single-arm phase II trial
Abstract
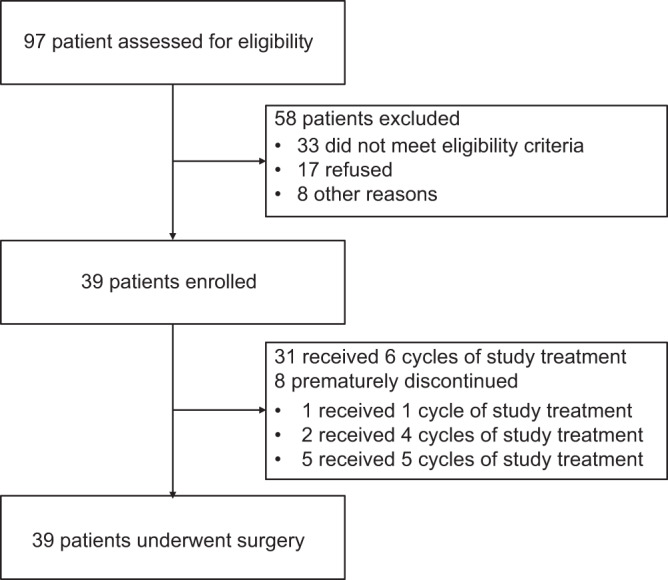
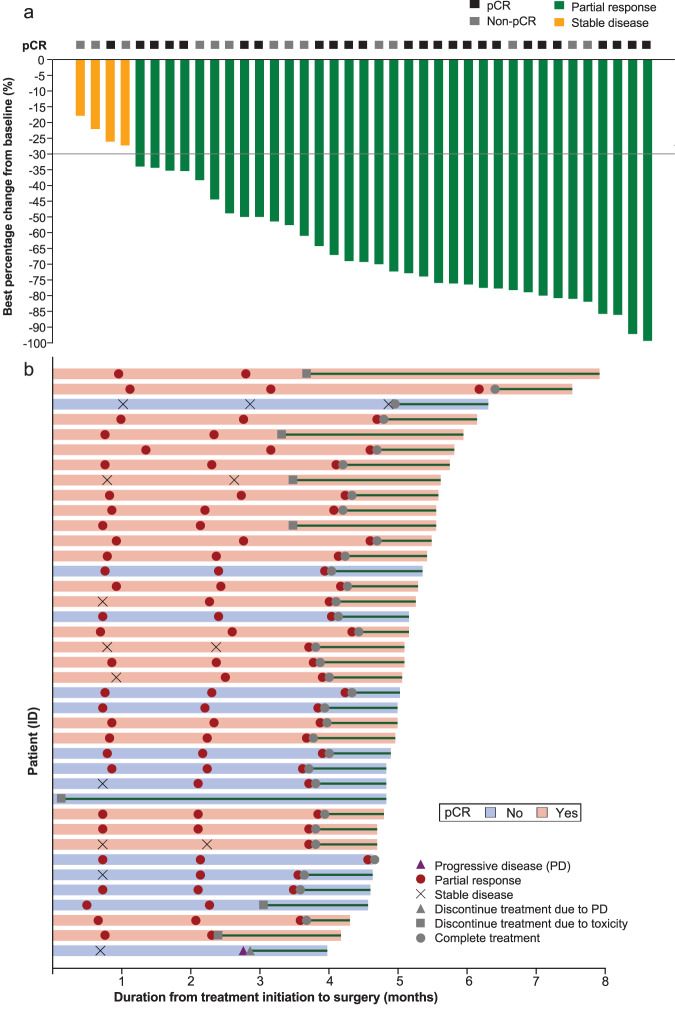
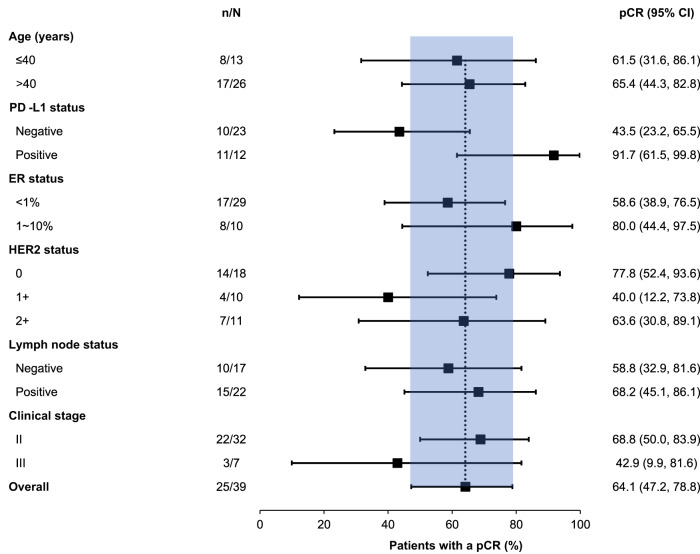
Immunotherapy combined with chemotherapy has been demonstrated to be effective in early triple-negative breast cancer (TNBC). In this single-arm, phase II study with Simon's two-stage design, we investigated the efficacy and safety of neoadjuvant camrelizumab plus chemotherapy in patients with early TNBC (NCT04213898). Eligible female patients aged 18 years or older with histologically confirmed treatment-naïve early TNBC were treated with camrelizumab (200 mg, on day 1), nab-paclitaxel (125 mg/m2, on days 1, 8, and 15), and epirubicin (75 mg/m2, on day 1) every three weeks for six cycles. The primary end point was the pathological complete response; secondary endpoints included safety, objective response rate, and long-term survival outcomes of event-free survival, disease-free survival, and distant disease-free survival. A total of 39 patients were enrolled between January 2020 and October 2021. Twenty-five patients achieved a pathological complete response (64.1%, 95%CI: 47.2, 78.8). The objective response rate was 89.7% (95%CI: 74.8, 96.7), including 35 patients with partial responses. Treatment-related adverse events of grade 3 or 4 occurred in 30 (76.9%) patients. In conclusion, the trial meets the prespecified endpoints showing promising efficacy and manageable safety of neoadjuvant camrelizumab plus nab-paclitaxel and epirubicin chemotherapy in female patients with early TNBC. Long-term survival outcomes are still pending.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
