

The effect of spinal versus general anaesthesia on perioperative muscle weakness in patients having bilateral total hip arthroplasty: a single center randomized clinical trial
- PMID: 37864209
- PMCID: PMC10588152
- DOI: 10.1186/s40001-023-01435-6
The effect of spinal versus general anaesthesia on perioperative muscle weakness in patients having bilateral total hip arthroplasty: a single center randomized clinical trial
Abstract
Background: Perioperative neuro-endocrine stress response may contribute to acquired muscle weakness. Regional anaesthesia has been reported to improve the outcome of patients having total hip arthroplasty. In this study, it was hypothesized that spinal anaesthesia (SA) decreases the perioperative neuro-endocrine stress response and perioperatively acquired muscle weakness (PAMW), as compared to general anaesthesia (GA).
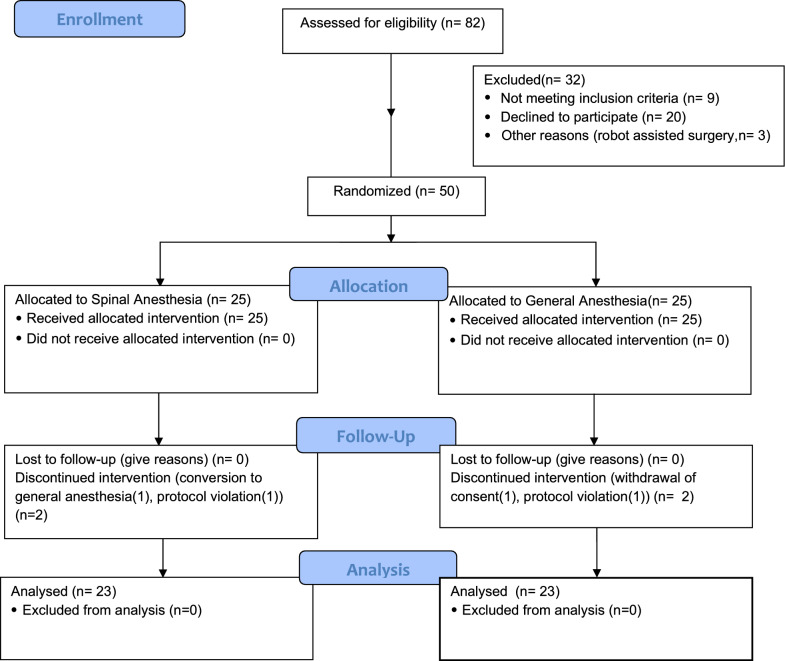
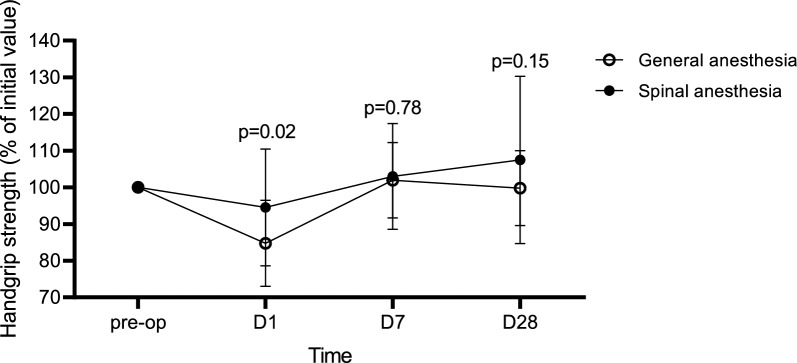
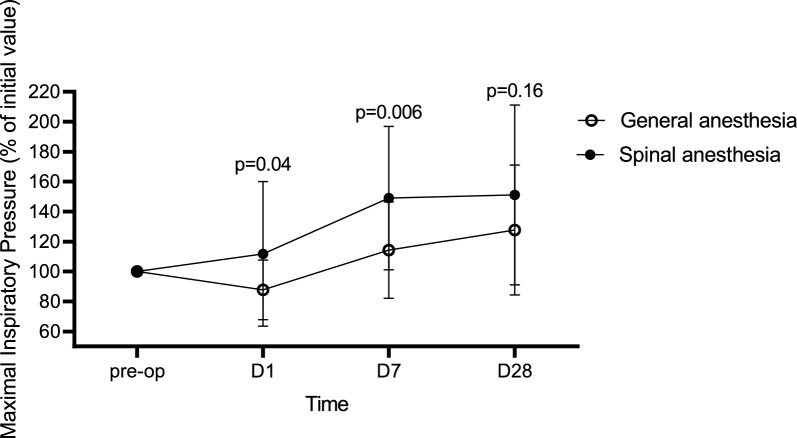
Methods: Fifty subjects undergoing bilateral total hip arthroplasty (THA) were randomly allocated to receive a standardized SA (n = 25) or GA (n = 25). Handgrip strength was assessed preoperatively, on the first postoperative day (primary endpoint) and on day 7 and 28. Respiratory muscle strength was measured by maximal inspiratory pressure (MIP). Stress response was assessed by measuring levels of Adrenocorticotropic hormone (ACTH), cortisol and interleukin-6 (IL-6).
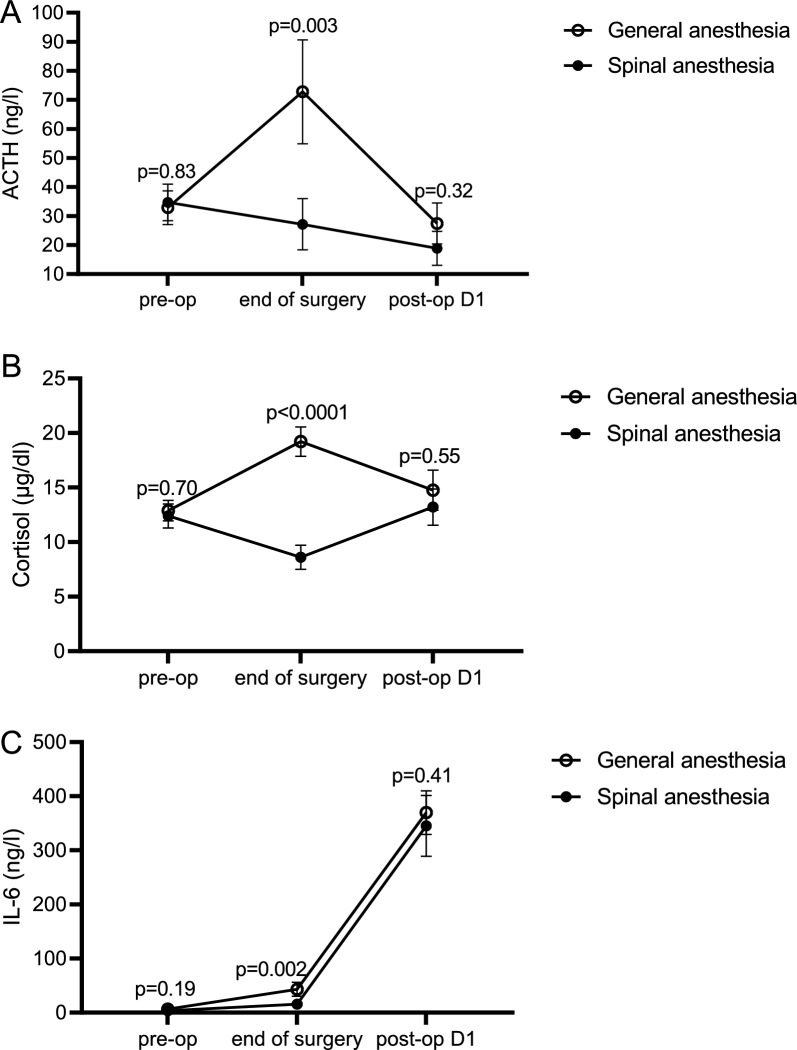
Results: Handgrip strength postoperatively (day 1) decreased by 5.4 ± 15.9% in the SA group, versus 15.2 ± 11.7% in the GA group (p = 0.02). The handgrip strength returned to baseline at day 7 and did not differ between groups at day 28. MIP increased postoperatively in patients randomized to SA by 11.7 ± 48.3%, whereas it decreased in GA by 12.2 ± 19.9% (p = 0.04). On day 7, MIP increased in both groups, but more in the SA (49.0 ± 47.8%) than in the GA group (14.2 ± 32.1%) (p = 0.006). Postoperatively, the levels of ACTH, cortisol and IL-6 increased in the GA, but not in the SA group (p < 0.004).
Conclusion: In patients having bilateral THA, SA preserved the postoperative respiratory and peripheral muscle strength and attenuated the neuro-endocrine and inflammatory responses.
Trial registration: clinicaltrials.gov NCT03600454.
Keywords: Bilateral total hip arthroplasty; General anaesthesia; Neuro-endocrine stress response; Perioperative muscle weakness; Spinal anaesthesia.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
AH has consulted, advised and/or performed industry-sponsored research for Philipps, GE, Sonosite, Konica Minolta, Codman & Shurtleff, Inc (Johnson and Johnson), Cadence, Insitu Biologics, Heron Therapeutics, Pacira, Baxter and BBraun Medical. Dr. Hadzic receives royalty income from BBraun Medical. He owns and directs NYSORA, the New York School of Regional Anesthesia. The other authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
