

The microbial metabolite desaminotyrosine enhances T-cell priming and cancer immunotherapy with immune checkpoint inhibitors
- PMID: 37865045
- PMCID: PMC10597767
- DOI: 10.1016/j.ebiom.2023.104834
The microbial metabolite desaminotyrosine enhances T-cell priming and cancer immunotherapy with immune checkpoint inhibitors
Abstract
Background: Inter-individual differences in response to immune checkpoint inhibitors (ICI) remain a major challenge in cancer treatment. The composition of the gut microbiome has been associated with differential ICI outcome, but the underlying molecular mechanisms remain unclear, and therapeutic modulation challenging.
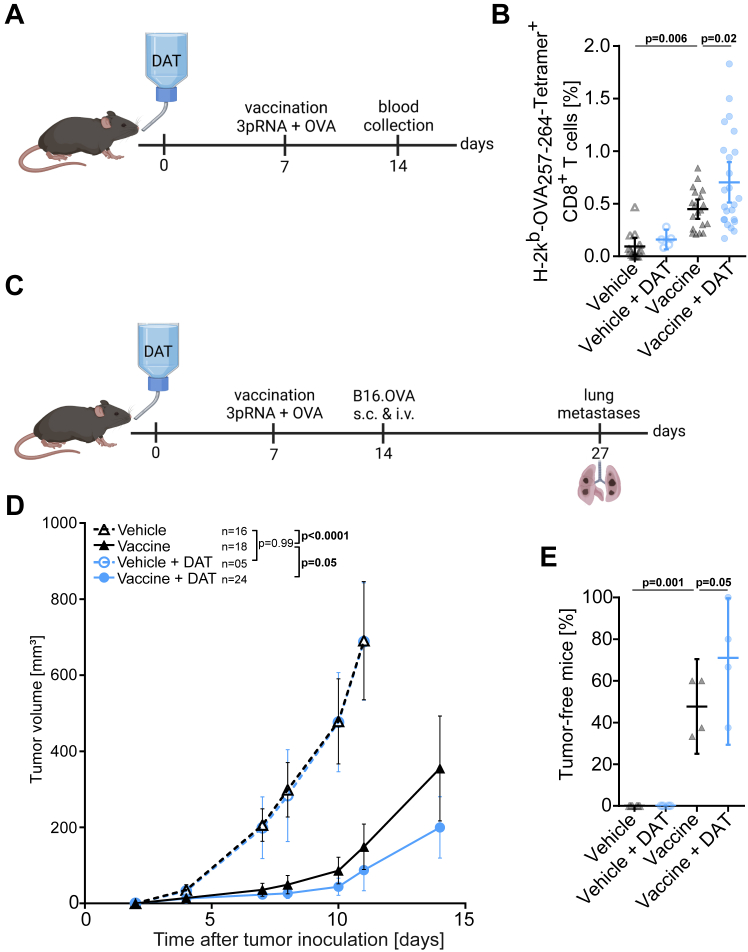
Methods: We established an in vivo model to treat C57Bl/6j mice with the type-I interferon (IFN-I)-modulating, bacterial-derived metabolite desaminotyrosine (DAT) to improve ICI therapy. Broad spectrum antibiotics were used to mimic gut microbial dysbiosis and associated ICI resistance. We utilized genetic mouse models to address the role of host IFN-I in DAT-modulated antitumour immunity. Changes in gut microbiota were assessed using 16S-rRNA sequencing analyses.
Findings: We found that oral supplementation of mice with the microbial metabolite DAT delays tumour growth and promotes ICI immunotherapy with anti-CTLA-4 or anti-PD-1. DAT-enhanced antitumour immunity was associated with more activated T cells and natural killer cells in the tumour microenvironment and was dependent on host IFN-I signalling. Consistent with this, DAT potently enhanced expansion of antigen-specific T cells following vaccination with an IFN-I-inducing adjuvant. DAT supplementation in mice compensated for the negative effects of broad-spectrum antibiotic-induced dysbiosis on anti-CTLA-4-mediated antitumour immunity. Oral administration of DAT altered the gut microbial composition in mice with increased abundance of bacterial taxa that are associated with beneficial response to ICI immunotherapy.
Interpretation: We introduce the therapeutic use of an IFN-I-modulating bacterial-derived metabolite to overcome resistance to ICI. This approach is a promising strategy particularly for patients with a history of broad-spectrum antibiotic use and associated loss of gut microbial diversity.
Funding: Melanoma Research Alliance, Deutsche Forschungsgemeinschaft, German Cancer Aid, Wilhelm Sander Foundation, Novartis Foundation.
Keywords: Antibiotics; Desaminotyrosine; Gut microbiome; Immune checkpoint inhibitors; Melanoma; Microbial metabolites.
Copyright © 2023 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests S.H. is a consultant for Bristol Myers-Squibb, Novartis, Merck, Abbvie, and Roche. S.H. has received research funding from Bristol Myers-Squibb and Novartis. H.P. is a consultant for Gilead, Abbvie, Pfizer, Novartis, Servier, and Bristol Myers-Squibb. K.S. is consultant for TRIMT GmbH and has filed a patent for radiopharmaceutical target. H.P. and S.H. have received research funding from Bristol Myers-Squibb. E.T.O. has received honoraria from BeiGene. C.P. received research funding from Almirall and honoraria from MSD, BMS, Pierre-Fabre, Sanofi, Novartis, Almirall, Pelpharma, Pritzer, Merck, Leo Pharma, Sun Pharma, Janssen, Abbvie, Amazentis, and Scarletred. S.H. is an employee of and holds equity interest in Roche/Genentech. The remaining authors declare no financial conflict of interest.
Figures






References
-
- Pires da Silva I., Ahmed T., Reijers I.L.M., et al. Ipilimumab alone or ipilimumab plus anti-PD-1 therapy in patients with metastatic melanoma resistant to anti-PD-(L)1 monotherapy: a multicentre, retrospective, cohort study. Lancet Oncol. 2021;22:836–847. doi: 10.1016/S1470-2045(21)00097-8. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
