Hyperactive delirium during emergency department stay: analysis of risk factors and association with short-term outcomes
- PMID: 37865623
- PMCID: PMC10954855
- DOI: 10.1007/s11739-023-03440-3
Hyperactive delirium during emergency department stay: analysis of risk factors and association with short-term outcomes
Abstract
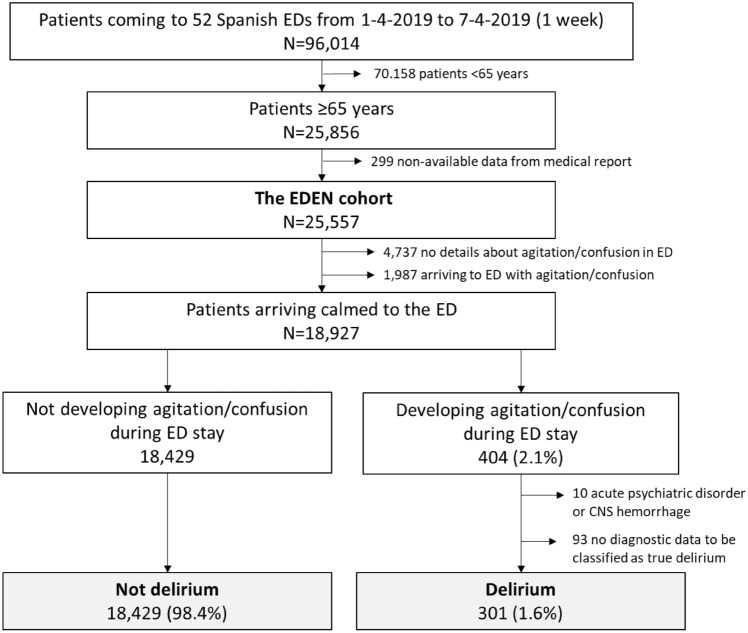
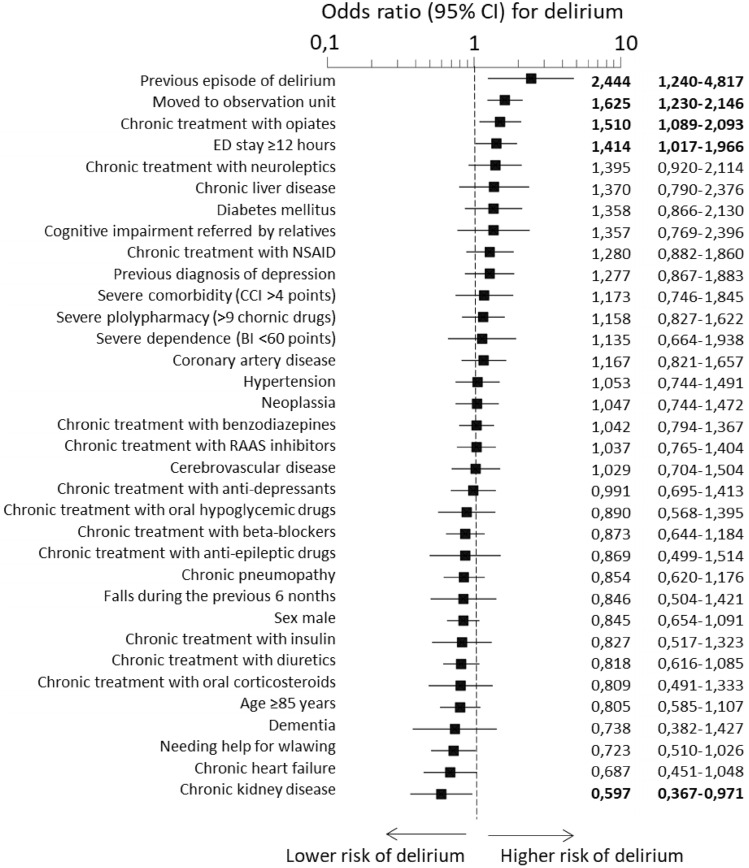
To investigate factors related to the development of hyperactive delirium in patients during emergency department (ED) stay and the association with short-term outcomes. A secondary analysis of the EDEN (Emergency Department and Elderly Needs) multipurpose multicenter cohort was performed. Patients older than 65 years arriving to the ED in a calm state and who developed confusion and/or psychomotor agitation requiring intravenous/intramuscular treatment during their stay in ED were assigned to delirium group. Patients with psychiatric and epileptic disorders and intracranial hemorrhage were excluded. Thirty-four variables were compared in both groups and outcomes were adjusted for age, sex, Charlson Comorbidity Index, Barthel Index and polypharmacy. Hyperactive delirium that needed treatment were developed in 301 out of 18,730 patients (1.6%). Delirium was directly associated with previous episodes of delirium (OR: 2.44, 95% CI 1.24-4.82), transfer to the ED observation unit (1.62, 1.23-2.15), chronic treatment with opiates (1.51, 1.09-2.09) and length of ED stay longer than 12 h (1.41, 1.02-1.97) and was indirectly associated with chronic kidney disease (0.60, 0.37-0.97). The 30-day all-cause mortality was 4.0% in delirium group and 2.9% in non-delirium group (OR: 1.52, 95% CI 0.83-2.78), need for hospitalization 25.6% and 25% (1.09, 0.83-1.43), in-hospital mortality 16.4% and 7.3% (2.32, 1.24-4.35), prolonged hospitalization 54.5% and 48.6% (1.27, 0.80-2.00), respectively, and 90-day post-discharge combined adverse event 36.4% and 35.8%, respectively (1.06, 0.82-2.00). Patients with previous episodes of delirium, treatment with opioids and longer stay in ED more frequently develop delirium during ED stay and preventive measures should be taken to minimize the incidence. Delirium is associated with in-hospital mortality during the index event.
Keywords: Benzodiazepines; Delirium; Emergency department; Mortality; Neuroleptics; Outcome.
© 2023. The Author(s).
Figures