

Skin-to-skin contact for the prevention of neonatal hypoglycaemia: a systematic review and meta-analysis
- PMID: 37865757
- PMCID: PMC10590034
- DOI: 10.1186/s12884-023-06057-8
Skin-to-skin contact for the prevention of neonatal hypoglycaemia: a systematic review and meta-analysis
Abstract
Background: Skin-to-skin contact between mother and infant after birth is recommended to promote breastfeeding and maternal-infant bonding. However, its impact on the incidence of neonatal hypoglycaemia is unknown. We conducted a systematic review and meta-analysis to assess this.
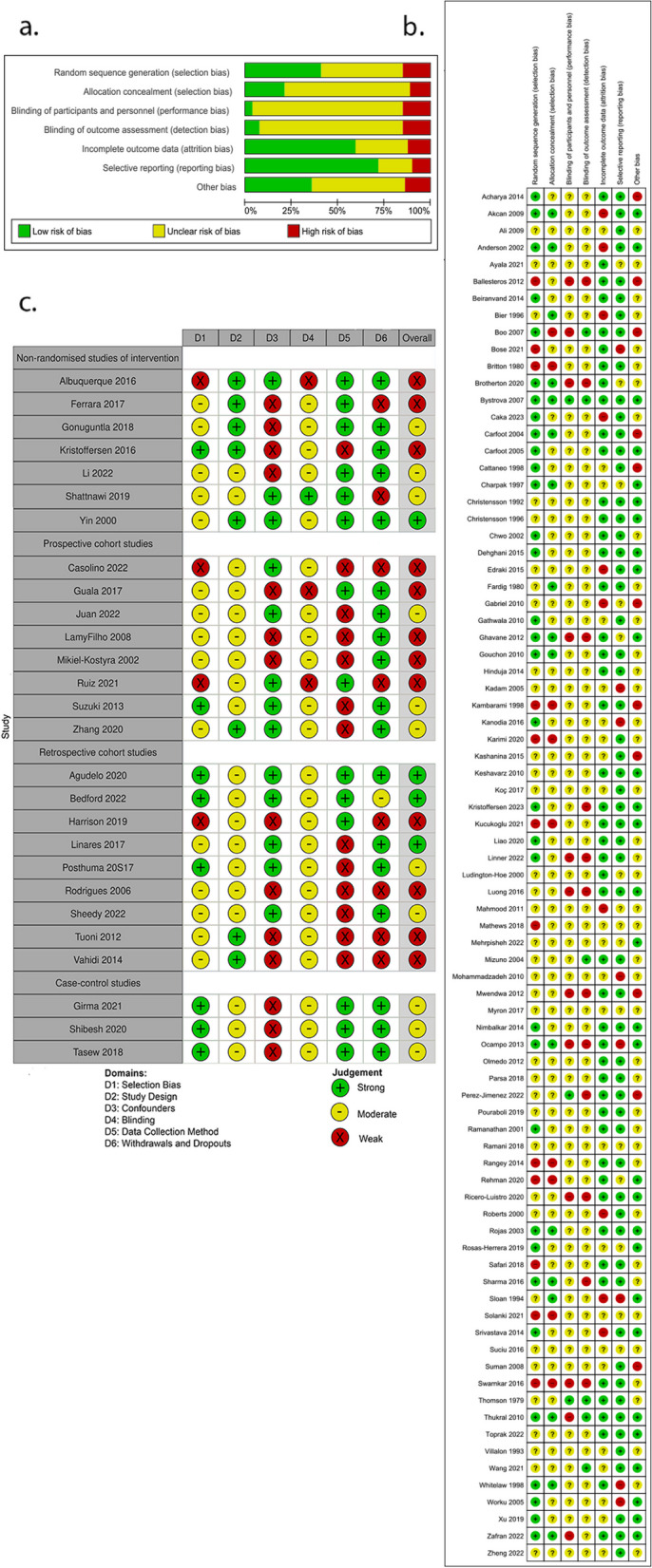
Methods: Published randomised control trials (RCTs), quasi-RCTs, non-randomised studies of interventions, cohort, or case-control studies with an intervention of skin-to-skin care compared to other treatment were included without language or date restrictions. The primary outcome was neonatal hypoglycaemia (study-defined). We searched 4 databases and 4 trial registries from inception to May 12th, 2023. Quality of studies was assessed using Cochrane Risk of Bias 1 or Effective Public Health Practice Project Quality Assessment tools. Certainty of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Results were synthesised using RevMan 5.4.1 or STATA and analysed using random-effects meta-analyses where possible, otherwise with direction of findings tables. This review was registered prospectively on PROSPERO (CRD42022328322).
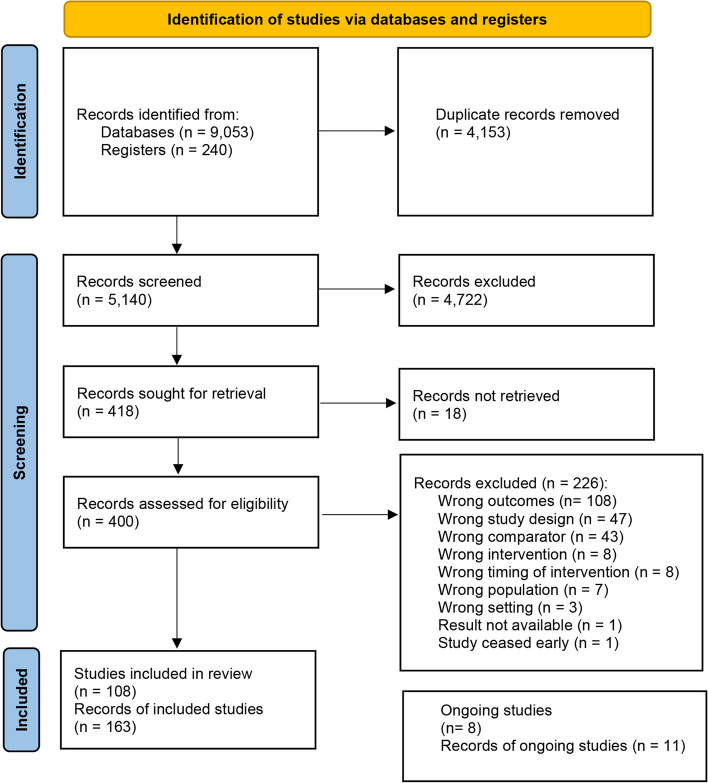
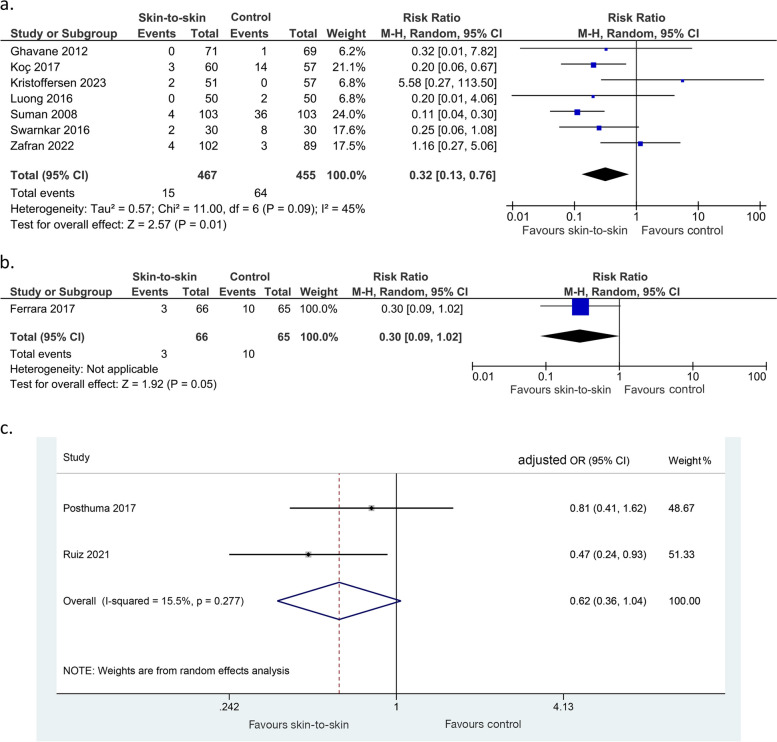
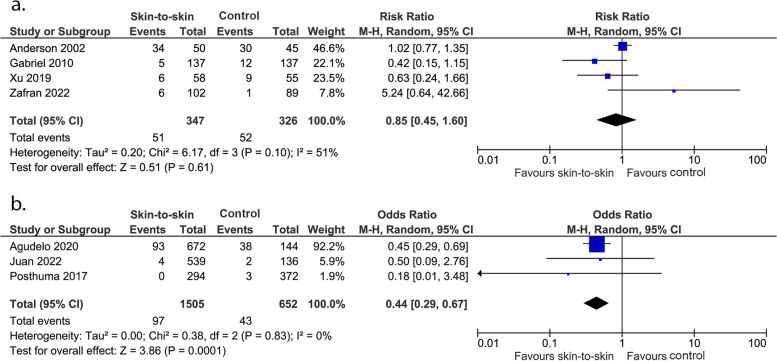
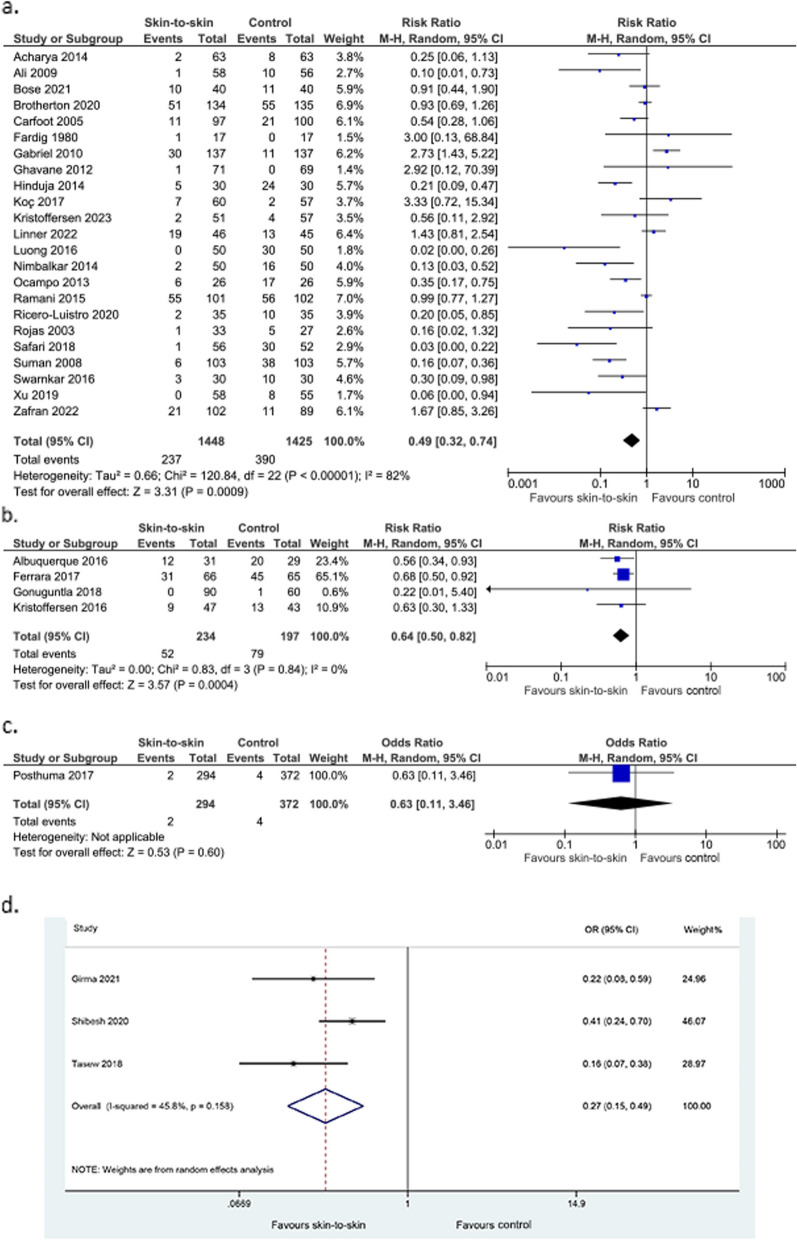
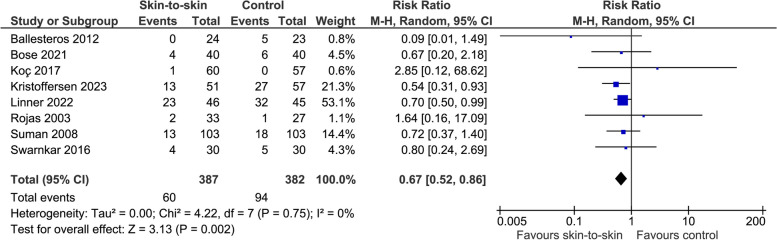
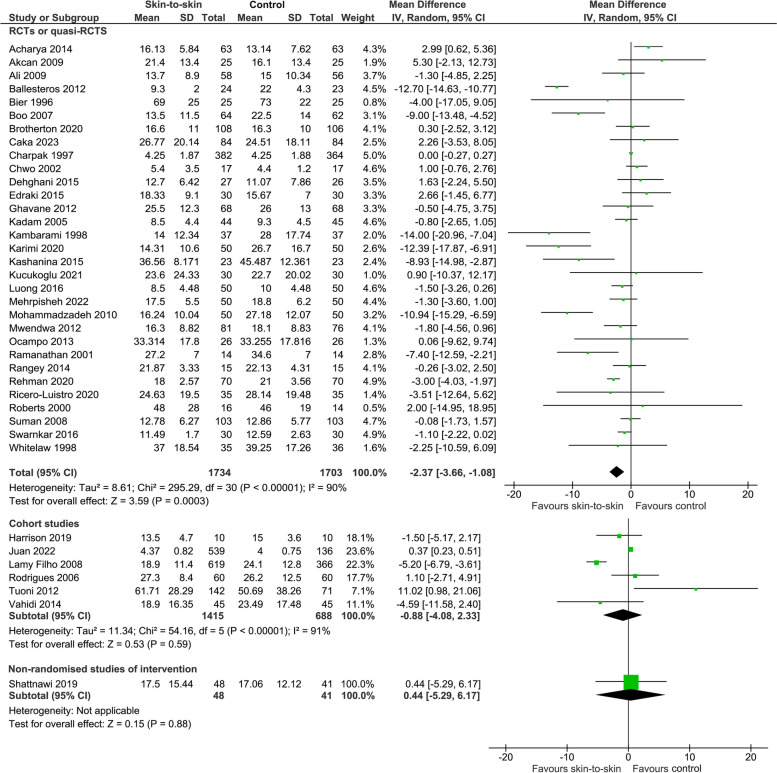
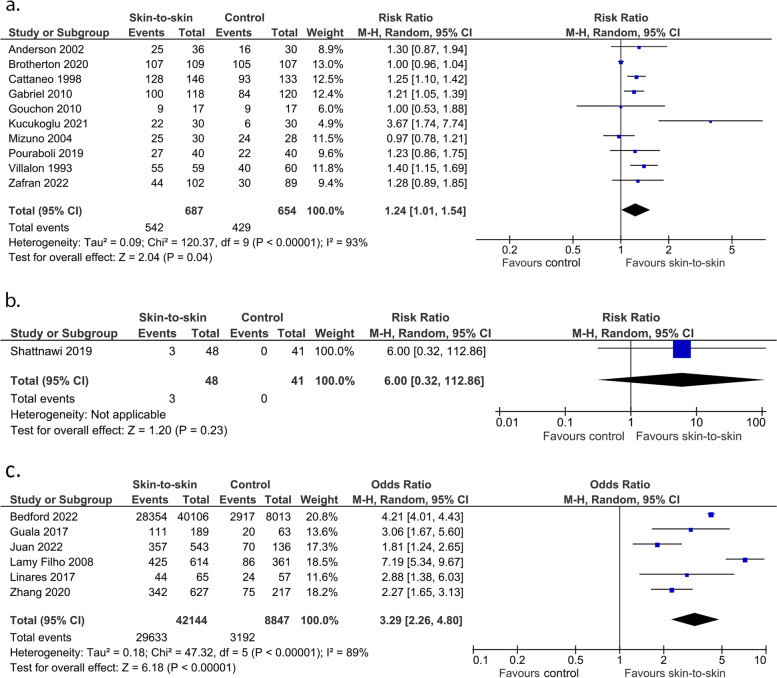
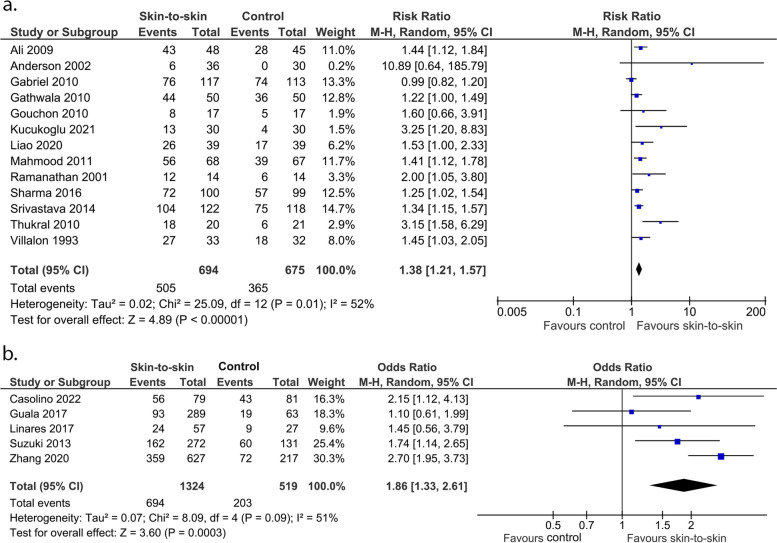
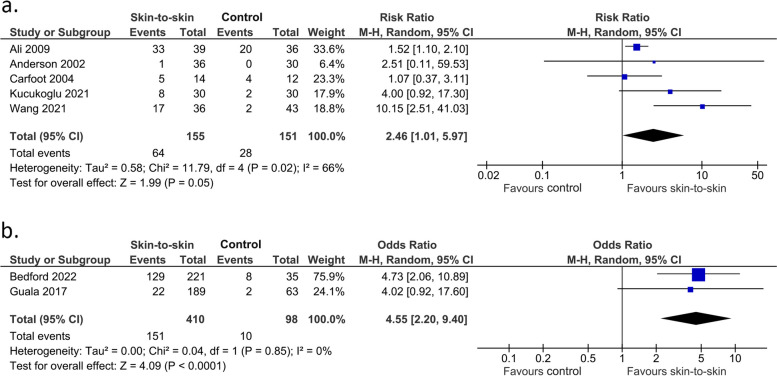
Results: This review included 84,900 participants in 108 studies, comprising 65 RCTs, 16 quasi-RCTs, seven non-randomised studies of intervention, eight prospective cohort studies, nine retrospective cohort studies and three case-control studies. Evidence suggests skin-to-skin contact may result in a large reduction in the incidence of neonatal hypoglycaemia (7 RCTs/quasi-RCTs, 922 infants, RR 0.29 (0.13, 0.66), p < 0.0001, I2 = 47%). Skin-to-skin contact may reduce the incidence of admission to special care or neonatal intensive care nurseries for hypoglycaemia (1 observational study, 816 infants, OR 0.50 (0.25-1.00), p = 0.050), but the evidence is very uncertain. Skin-to-skin contact may reduce duration of initial hospital stay after birth (31 RCTs, 3437 infants, MD -2.37 (-3.66, -1.08) days, p = 0.0003, I2 = 90%, p for Egger's test = 0.02), and increase exclusive breastmilk feeding from birth to discharge (1 observational study, 1250 infants, RR 4.30 (3.19, 5.81), p < 0.0001), but the evidence is very uncertain.
Conclusion: Skin-to-skin contact may lead to a large reduction in the incidence of neonatal hypoglycaemia. This, along with other established benefits, supports the practice of skin-to-skin contact for all infants and especially those at risk of hypoglycaemia.
Keywords: Hypoglycaemia; Infant; Kangaroo Mother Care; Kangaroo care; Neonatology; Newborn; Skin-to-skin.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Hay WW, Jr, Raju TN, Higgins RD, Kalhan SC, Devaskar SU. Knowledge gaps and research needs for understanding and treating neonatal hypoglycemia: workshop report from Eunice Kennedy Shriver National Institute of Child Health and Human Development. J Pediatr. 2009;155(5):612–617. doi: 10.1016/j.jpeds.2009.06.044. - DOI - PMC - PubMed
-
- Starship Child Health. Hypoglycaemia in the neonate Auckland (NZ): Starship Child Health; 2019. Available from: https://starship.org.nz/guidelines/hypoglycaemia-in-the-neonate/
-
- UNICEF. Skin-to-skin contact [place unknown]: [publisher unknown]; [date unknown]. Available from: https://www.unicef.org.uk/babyfriendly/baby-friendly-resources/implement...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
