

Impact of stress hyperglycemia ratio on mortality in patients with critical acute myocardial infarction: insight from american MIMIC-IV and the chinese CIN-II study
- PMID: 37865764
- PMCID: PMC10589959
- DOI: 10.1186/s12933-023-02012-1
Impact of stress hyperglycemia ratio on mortality in patients with critical acute myocardial infarction: insight from american MIMIC-IV and the chinese CIN-II study
Abstract
Background: Among patients with acute coronary syndrome and percutaneous coronary intervention, stress hyperglycemia ratio (SHR) is primarily associated with short-term unfavorable outcomes. However, the relationship between SHR and long-term worsen prognosis in acute myocardial infarction (AMI) patients admitted in intensive care unit (ICU) are not fully investigated, especially in those with different ethnicity. This study aimed to clarify the association of SHR with all-cause mortality in critical AMI patients from American and Chinese cohorts.
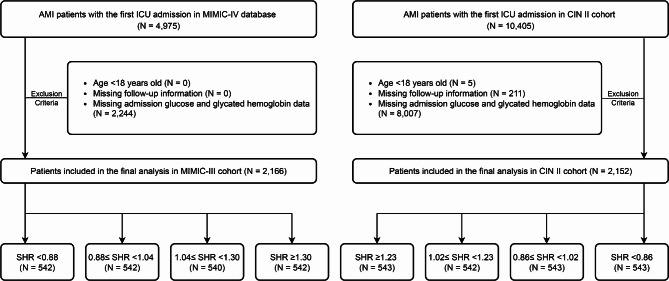
Methods: Overall 4,337 AMI patients with their first ICU admission from the American Medical Information Mart for Intensive Care (MIMIC)-IV database (n = 2,166) and Chinese multicenter registry cohort Cardiorenal ImprovemeNt II (CIN-II, n = 2,171) were included in this study. The patients were divided into 4 groups based on quantiles of SHR in both two cohorts.
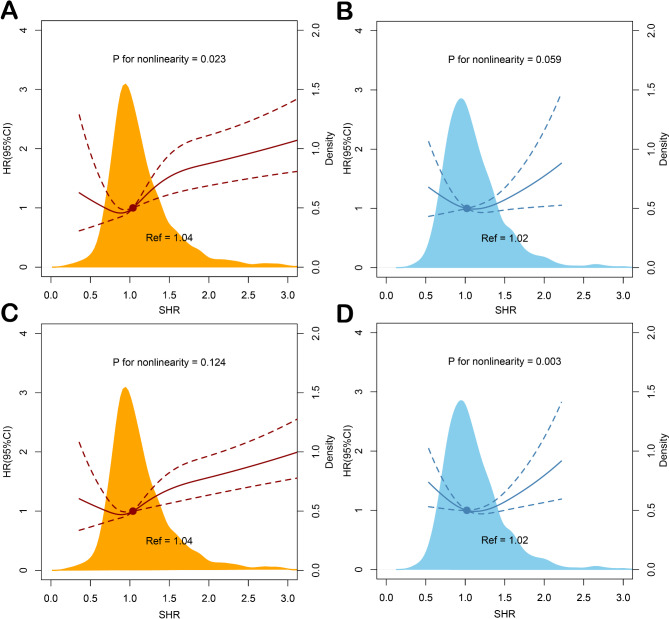
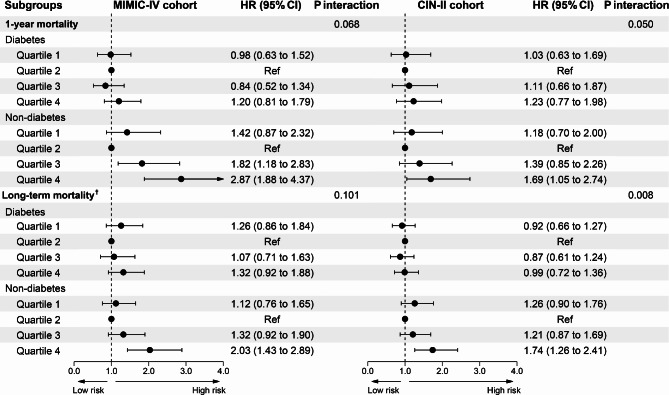
Results: The total mortality was 23.8% (maximum follow-up time: 12.1 years) in American MIMIC-IV and 29.1% (maximum follow-up time: 14.1 years) in Chinese CIN-II. In MIMIC-IV cohort, patients with SHR of quartile 4 had higher risk of 1-year (adjusted hazard radio [aHR] = 1.87; 95% CI: 1.40-2.50) and long-term (aHR = 1.63; 95% CI: 1.27-2.09) all-cause mortality than quartile 2 (as reference). Similar results were observed in CIN-II cohort (1-year mortality: aHR = 1.44; 95%CI: 1.03-2.02; long-term mortality: aHR = 1.32; 95%CI: 1.05-1.66). In both two group, restricted cubic splines indicated a J-shaped correlation between SHR and all-cause mortality. In subgroup analysis, SHR was significantly associated with higher 1-year and long-term all-cause mortality among patients without diabetes in both MIMIC-IV and CIN-II cohort.
Conclusion: Among critical AMI patients, elevated SHR is significantly associated with and 1-year and long-term all-cause mortality, especially in those without diabetes, and the results are consistently in both American and Chinese cohorts.
Keywords: Coronary artery disease; Diabetes; Mortality; Stress hyperglycemia ratio.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
