

A modified prosthesis eversion technique for proximal anastomosis in ascending aorta replacement
- PMID: 37868872
- PMCID: PMC10586958
- DOI: 10.21037/jtd-23-550
A modified prosthesis eversion technique for proximal anastomosis in ascending aorta replacement
Abstract
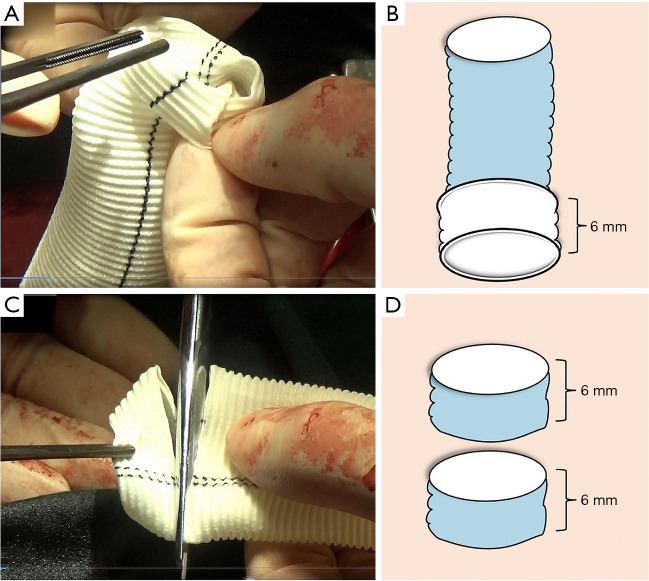
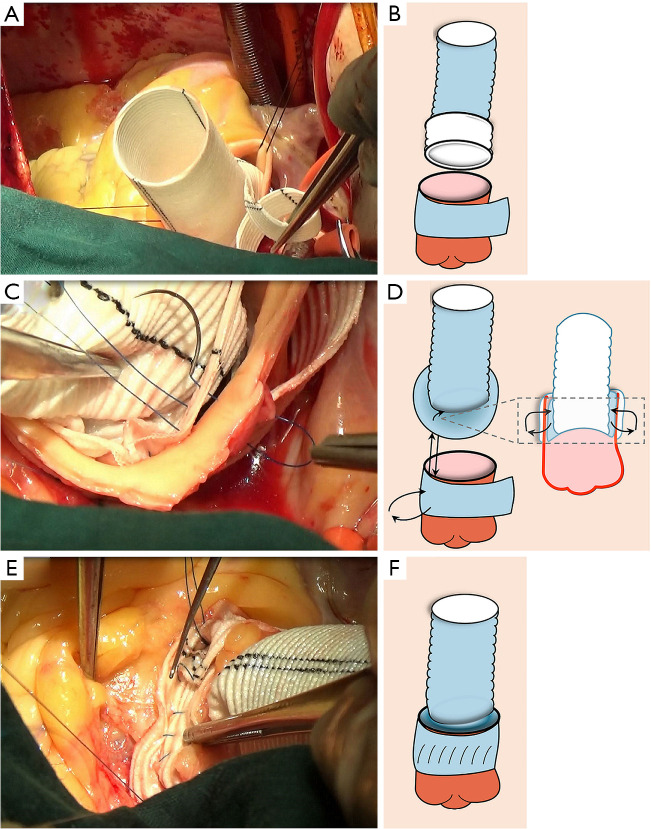
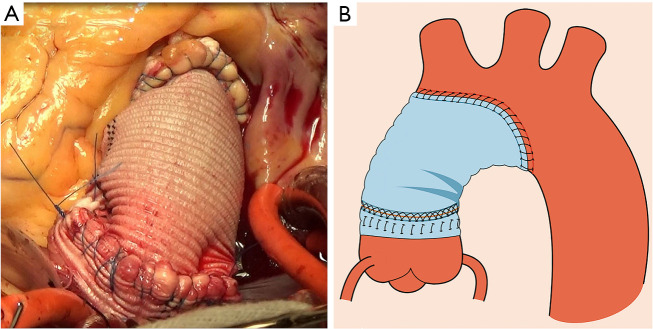
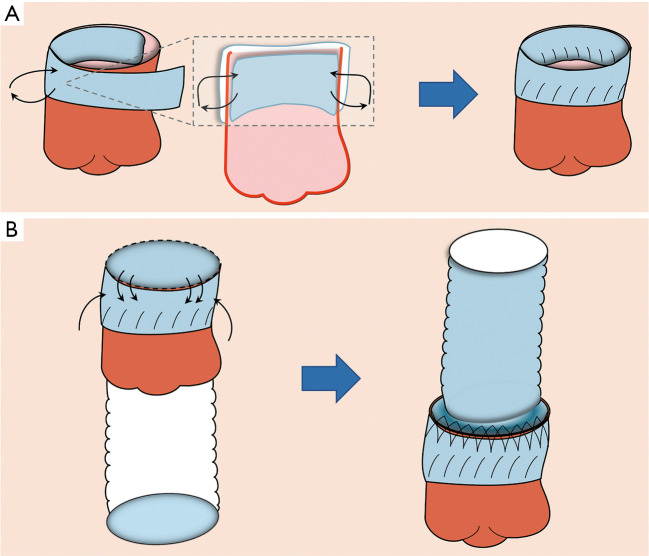
Background: One of the crucial aspects of ascending aorta replacement is to achieve hemostasis of the proximal anastomosis. This study aimed to describe a modified prosthesis eversion technique for proximal anastomosis in ascending aorta replacement and compare its operative outcomes with the conventional prosthesis eversion technique.
Methods: We conducted a retrospective analysis of all consecutive patients who had ascending aortic aneurysm and underwent ascending aorta replacement with the modified or conventional prosthesis eversion technique between January 2019 and December 2022 in our center.
Results: A total of 108 patients were included: 55 in the modified group and 53 in the conventional group. The durations of cardiopulmonary bypass, aortic cross-clamping and total operation in the conventional group were longer than those in the modified group. Furthermore, perioperative blood loss and the incidence of re-exploration for bleeding were significantly lower in the modified group. Accordingly, patients in the conventional group accepted more blood transfusion. The modified group had a shorter duration in intensive care unit (ICU) and hospital, and lower total hospitalization costs than those in the conventional group.
Conclusions: The modified prosthesis eversion technique is an effective alternative for proximal anastomosis in ascending aorta replacement, with less blood loss, shorter operation time, and lower rate of postoperative complications compared with the conventional technique.
Keywords: Prosthesis eversion; ascending aorta replacement; clinical outcomes; proximal anastomosis.
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-550/coif). The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources