

Successful repair of acquired intrathoracic nonmalignant tracheoesophageal fistulas using thoracoacromial artery perforator flap through a midsternal incision approach: a report of three cases
- PMID: 37868901
- PMCID: PMC10586943
- DOI: 10.21037/jtd-23-1128
Successful repair of acquired intrathoracic nonmalignant tracheoesophageal fistulas using thoracoacromial artery perforator flap through a midsternal incision approach: a report of three cases
Abstract
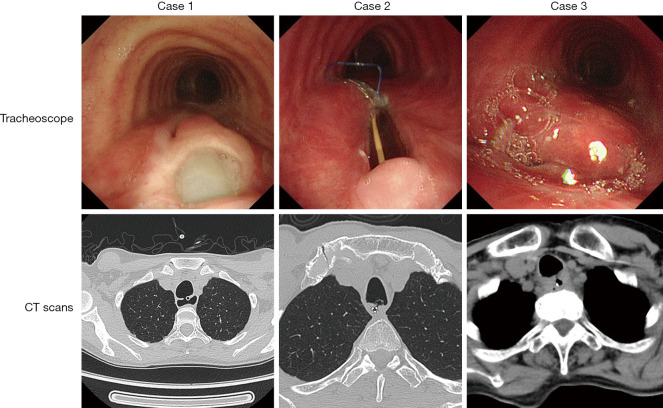
Background: Acquired intrathoracic nonmalignant tracheoesophageal fistulas (TEFs) are rare and challenging surgical problems. They can constitute a life-threatening condition due to severe pulmonary complications and poor nutrition. Surgical treatment is effective for most patients undergoing operative repair. However, in recent studies, the difficult-to-ignore early complications of surgical treatment can be as high as 62.5%. Among them, esophageal stricture occurring in 42-54% of patients, anastomosis leakage occurs at a rate of 22.7-26%, and the mortality rate can be as high as 29.4%. Here, we introduce our innovative experience repairing acquired TEFs with a thoracoacromial artery perforator flap, in which provides a clear surgical field of view, reliable reconstruction, and no serious complications during the perioperative period and no mortality or complications were observed within 180 days after the operation.
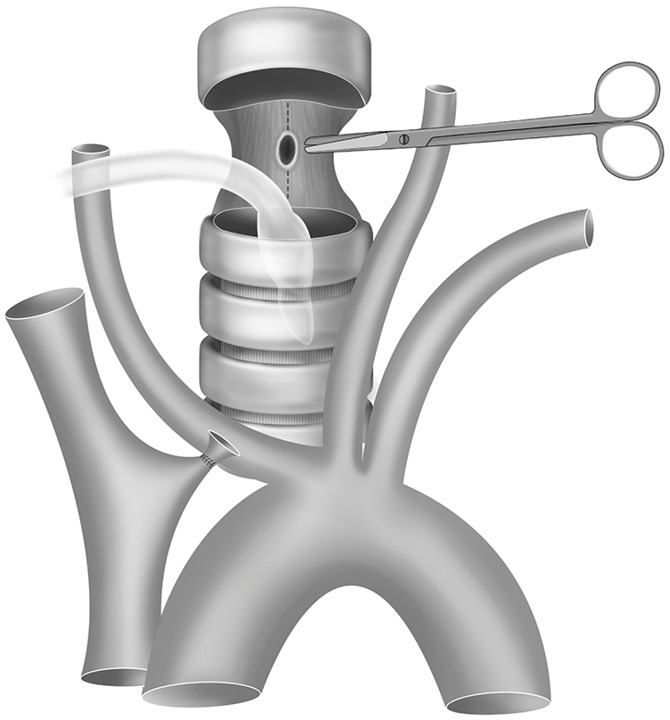
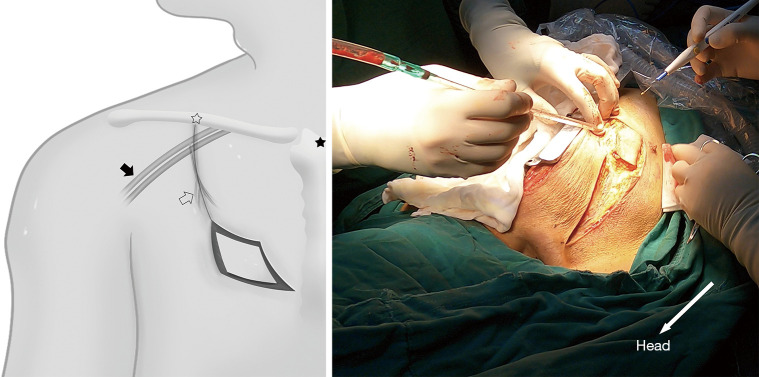
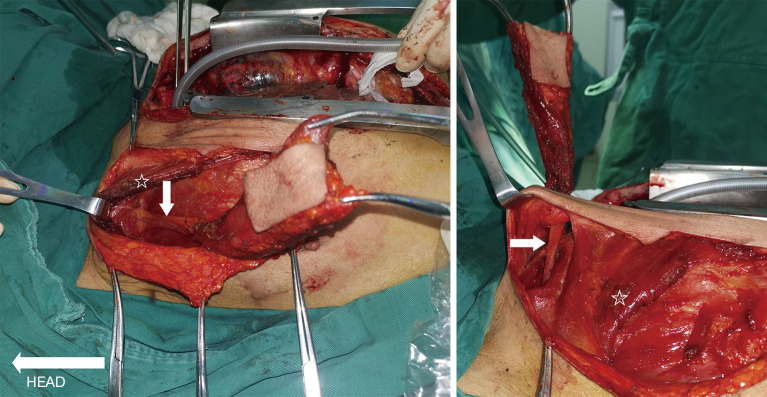
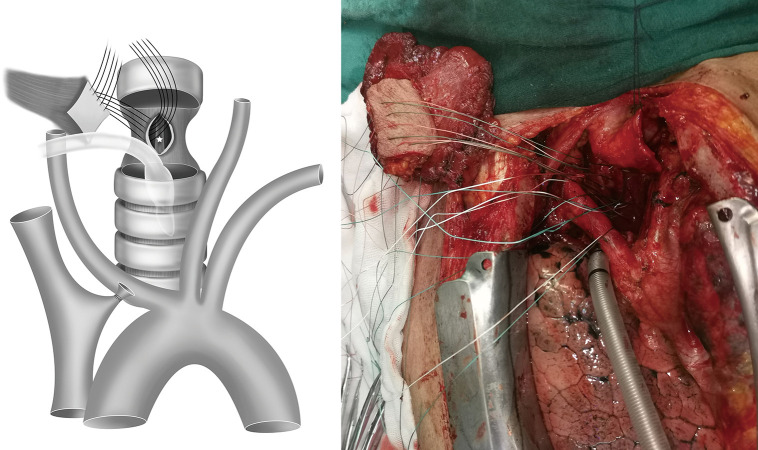
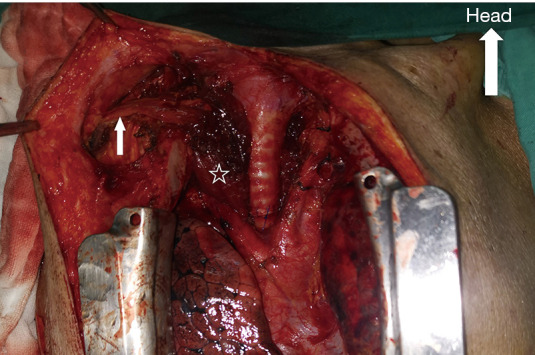
Case description: Surgical repair with a thoracoacromial artery perforator flap through a midsternal incision approach was performed in 3 patients. During the procedure, a midsternal incision was made. After the thymus and anterior mediastinal fat were resected, and the left innominate vein was transected, the trachea and esophagus were mobilized. The trachea was incised and pulled to the cranial and caudal sides. Then, the thoracoacromial artery perforator flap was harvested and transferred into the superior mediastinum for esophageal reconstruction. Subsequently, the trachea was anastomosed end to end after debridement, and the left innominate vein was either anastomosed or not. Two patients developed esophageal anastomotic leakage postoperatively and healed well after nonsurgical treatment. No mortality or other complications were observed at 180 days after the operation.
Conclusions: Repair of acquired TEFs using a thoracoacromial artery perforator flap through a midsternal incision approach is an effective, safe surgical treatment.
Keywords: Tracheoesophageal fistulas (TEFs); case report; thoracoacromial artery perforator flap (TAPF).
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-23-1128/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Boybeyi-Turer O, Soyer T. Tracheoesophageal fistula after esophageal atresia repair: recurrent, missed or acquired. Curr Chall Thorac Surg 2022;4:26. 10.21037/ccts-20-166 - DOI
Publication types
LinkOut - more resources
Full Text Sources