

Effect of newly developed scissors-attached micro-forceps on the recipient clamp time and occurrence of anastomotic site infarction after bypass surgery for moyamoya disease
- PMID: 37869149
- PMCID: PMC10587554
- DOI: 10.3389/fneur.2023.1269400
Effect of newly developed scissors-attached micro-forceps on the recipient clamp time and occurrence of anastomotic site infarction after bypass surgery for moyamoya disease
Abstract
Introduction: This study aimed to examine the effect of newly developed scissors-attached micro-forceps in superficial temporal artery-to-middle cerebral artery (STA-MCA) anastomosis for moyamoya disease (MMD).
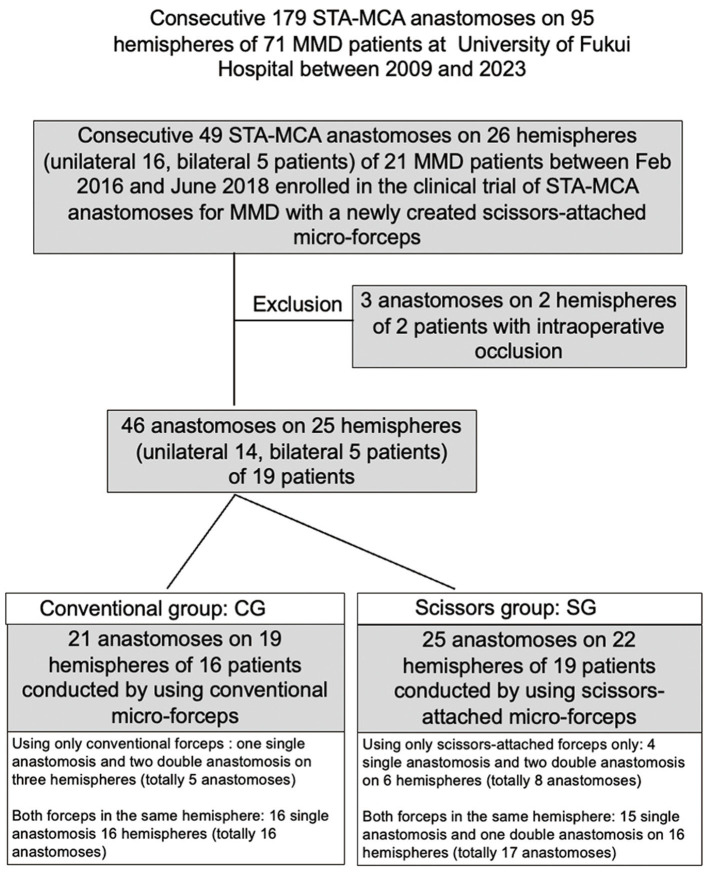
Materials and methods: Of 179 consecutive STA-MCA anastomoses on 95 hemispheres of 71 MMD patients at the University of Fukui Hospital between 2009 and 2023, 49 anastomoses on 26 hemispheres of 21 patients were enrolled in this retrospective cohort clinical trial intraoperative indocyanine green video-angiography did not demonstrate bypass patency in three anastomoses in two patients who were excluded. Twenty-one anastomosis in 19 hemispheres of 16 patients were performed using the conventional micro-forceps (conventional group, CG), and 25 anastomoses in 22 hemispheres of 19 patients were performed using scissors-attached micro-forceps (scissors group, SG). A small infarction near the anastomotic site detected using postoperative diffusion-weighted imaging was defined as anastomotic site infarction (ASI). Factors affecting the occurrence of ASI were examined by univariate, logistic regression, and receiver operating curve (ROC) analysis.
Results: There were no significant differences in clinical parameters such as age, sex, number of sacrificed branches, number of sacrificed large branches, and number of sutures between the CG and SG. However, the clamp time and occurrence of ASI were significantly lower in the SG than in the CG. Logistic regression analysis revealed that the clamp time was the only significant factor predicting the occurrence of ASI. A receiver operating curve analysis also revealed that the clamp time significantly predicted the occurrence of ASI (area under the curve, 0.875; cutoff value, 33.2 min).
Conclusion: The newly developed scissors-attached micro-forceps could significantly reduce the clamp time and occurrence of ASI in STA-MCA anastomosis for MMD.
Keywords: STA-MCA anastomosis; anastomotic site; clamp time; ischemia; micro-forceps; moyamoya disease.
Copyright © 2023 Yomo, Kitai, Tada, Isozaki, Higashino, Matsuda, Yamauchi, Akazawa, Kawajri, Oiwa, Yamada, Tsubota, Watanabe, Okazawa, Kiyono, Arishma and Kikuta.
Conflict of interest statement
HT was employed by Charmant Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Yasargil MG. Anastomosis between the superficial temporal artery and a branch of the middle cerebral artery. In:Yasargil MG, editor. Microsurgery Applied to Neurosurgery. Stuttgart: George Thieme Verlag; (1969). p. 105–15.
-
- Fujimura M, Tominaga T, Kuroda S, Takahashi JC, Endo H, Ogasawara K, et al. . (Spontaneous occlusion of circle of willis) of the Ministry of Health, Labor Welfare, Japan; Guideline Committee 2021 of the Japan Stroke Society. 2021 Japanese guidelines for the management of Moyamoya disease: guidelines from the research Committee on Moyamoya disease and Japan Stroke Society. Neurol Med Chir. (2022) 62:165–70. 10.2176/jns-nmc.2021-0382 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources