

Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial
- PMID: 37870536
- PMCID: PMC10730032
- DOI: 10.1200/JCO.23.02005
Efficacy and Safety of Trastuzumab Deruxtecan in Patients With HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial
Abstract
Purpose: Trastuzumab deruxtecan (T-DXd) is a human epidermal growth factor 2 (HER2)-directed antibody-drug conjugate approved in HER2-expressing breast and gastric cancers and HER2-mutant non-small-cell lung cancer. Treatments are limited for other HER2-expressing solid tumors.
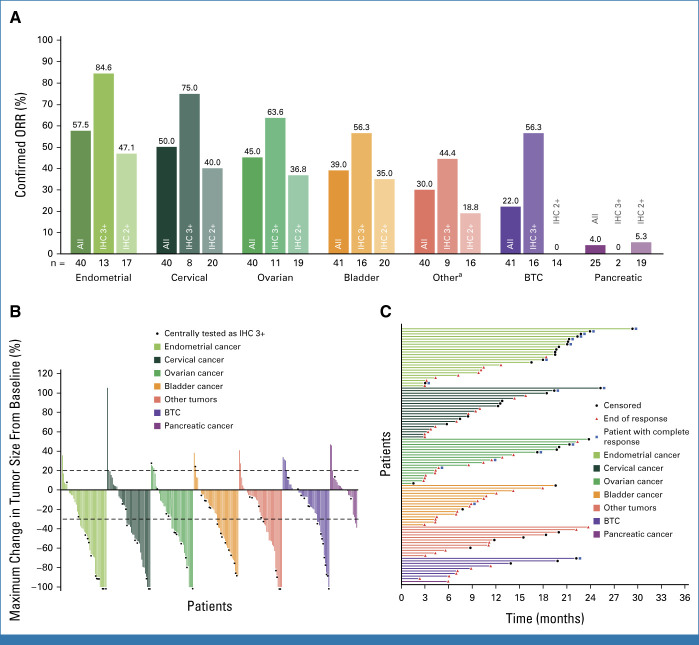
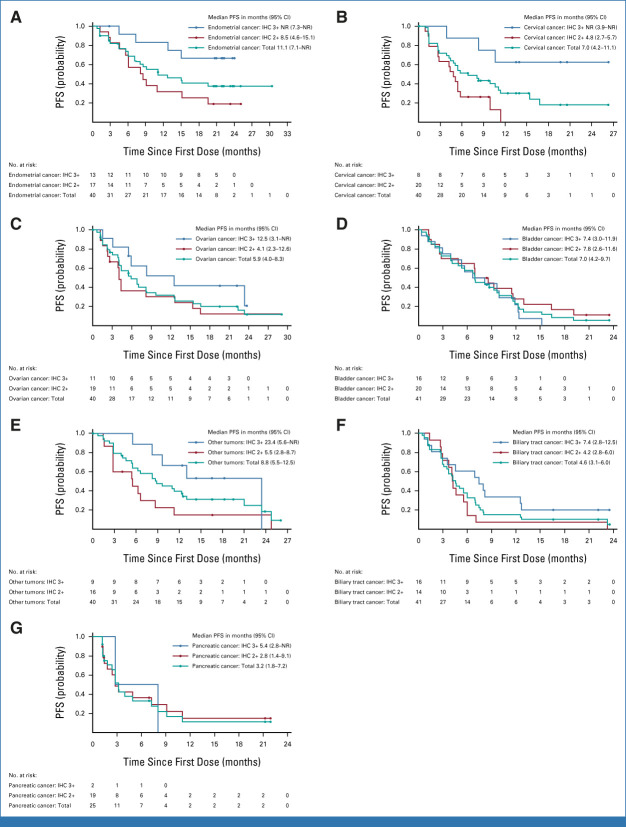
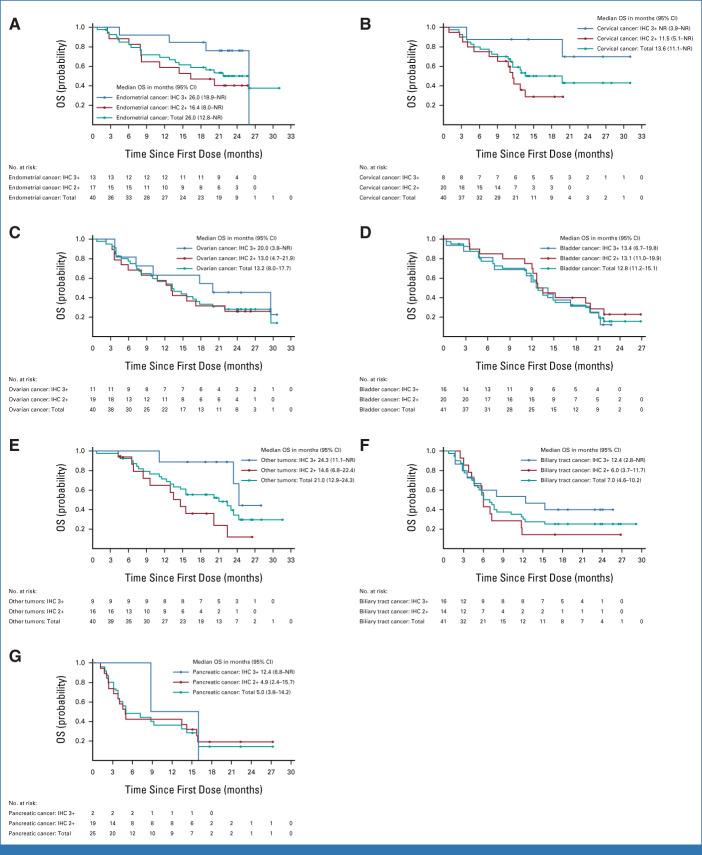
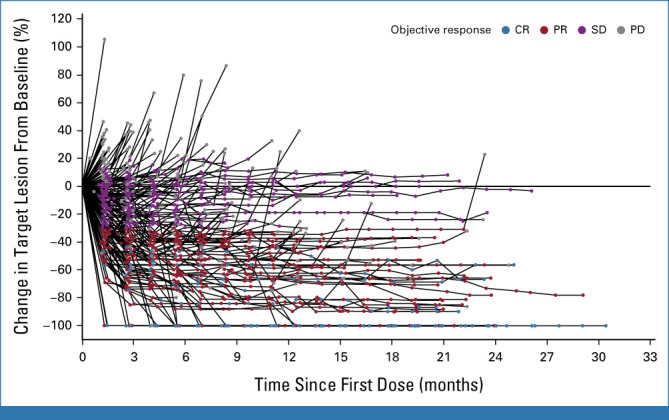
Methods: This open-label phase II study evaluated T-DXd (5.4 mg/kg once every 3 weeks) for HER2-expressing (immunohistochemistry [IHC] 3+/2+ by local or central testing) locally advanced or metastatic disease after ≥1 systemic treatment or without alternative treatments. The primary end point was investigator-assessed confirmed objective response rate (ORR). Secondary end points included safety, duration of response, progression-free survival (PFS), and overall survival (OS).
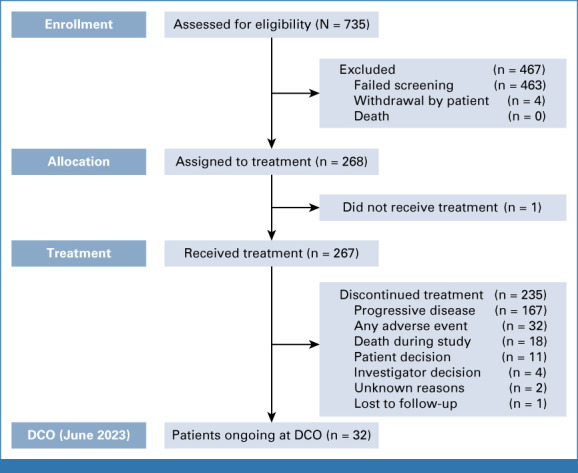
Results: At primary analysis, 267 patients received treatment across seven tumor cohorts: endometrial, cervical, ovarian, bladder, biliary tract, pancreatic, and other. The median follow-up was 12.75 months. In all patients, the ORR was 37.1% (n = 99; [95% CI, 31.3 to 43.2]), with responses in all cohorts; the median DOR was 11.3 months (95% CI, 9.6 to 17.8); the median PFS was 6.9 months (95% CI, 5.6 to 8.0); and the median OS was 13.4 months (95% CI, 11.9 to 15.5). In patients with central HER2 IHC 3+ expression (n = 75), the ORR was 61.3% (95% CI, 49.4 to 72.4), the median DOR was 22.1 months (95% CI, 9.6 to not reached), the median PFS was 11.9 months (95% CI, 8.2 to 13.0), and the median OS was 21.1 months (95% CI, 15.3 to 29.6). Grade ≥3 drug-related adverse events were observed in 40.8% of patients; 10.5% experienced adjudicated drug-related interstitial lung disease (ILD), with three deaths.
Conclusion: Our study demonstrates durable clinical benefit, meaningful survival outcomes, and safety consistent with the known profile (including ILD) in pretreated patients with HER2-expressing tumors receiving T-DXd. Greatest benefit was observed for the IHC 3+ population. These data support the potential role of T-DXd as a tumor-agnostic therapy for patients with HER2-expressing solid tumors.
Trial registration: ClinicalTrials.gov NCT04482309.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
Comment in
-
Tumor-Agnostic Treatment Heading to the Clinic?Cancer Discov. 2023 Dec 12;13(12):OF10. doi: 10.1158/2159-8290.CD-ND2023-0013. Cancer Discov. 2023. PMID: 37888905
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
