Choosing Wisely interventions to reduce antibiotic overuse in the safety net
- PMID: 37870542
- PMCID: PMC10994234
- DOI: 10.37765/ajmc.2023.89367
Choosing Wisely interventions to reduce antibiotic overuse in the safety net
Abstract
Objectives: Physician pay-for-performance (P4P) programs frequently target inappropriate antibiotics. Yet little is known about P4P programs' effects on antibiotic prescribing among safety-net populations at risk for unintended harms from reducing care. We evaluated effects of P4P-motivated interventions to reduce antibiotic prescriptions for safety-net patients with acute respiratory tract infections (ARTIs).
Study design: Interrupted time series.
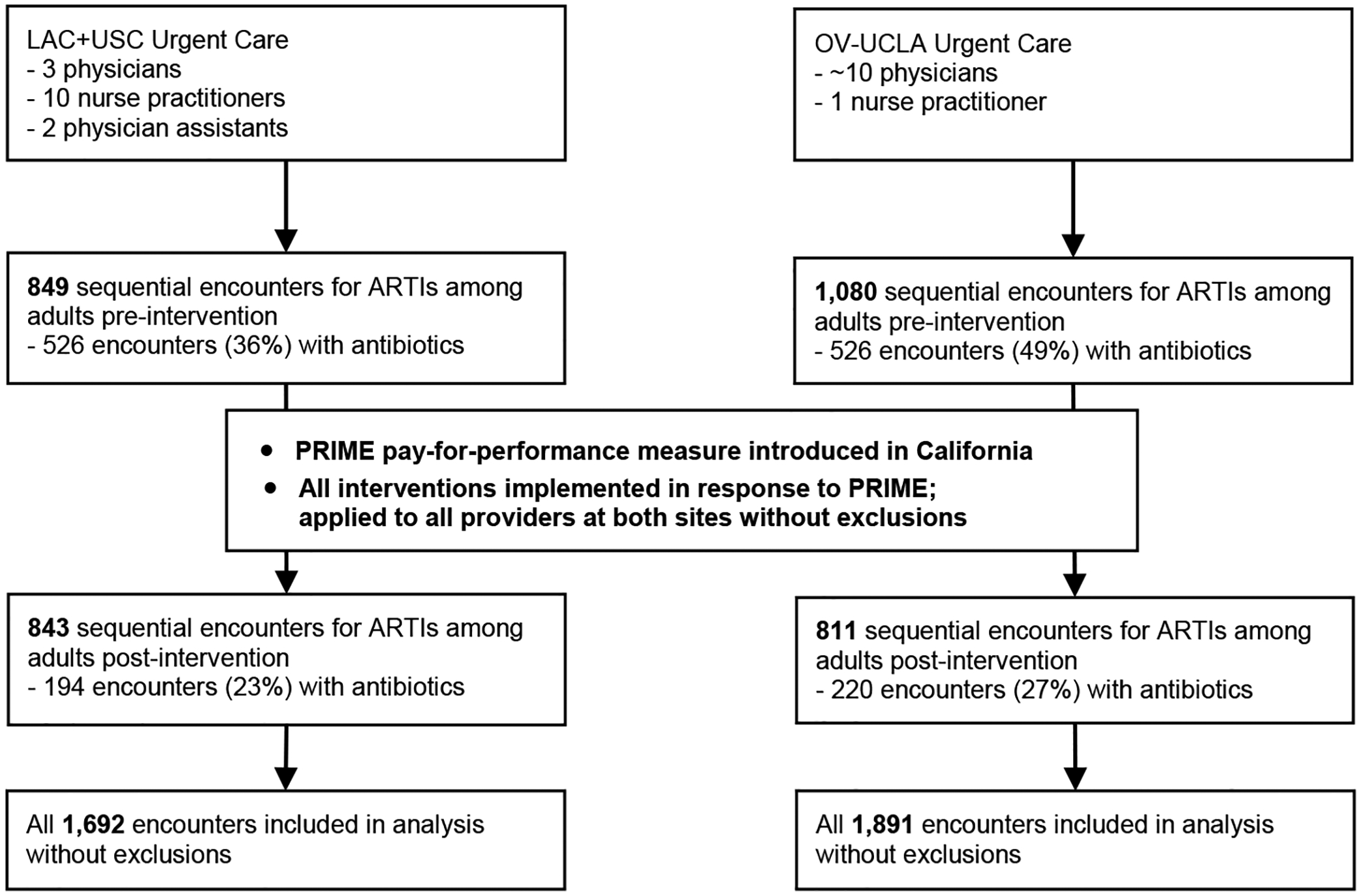
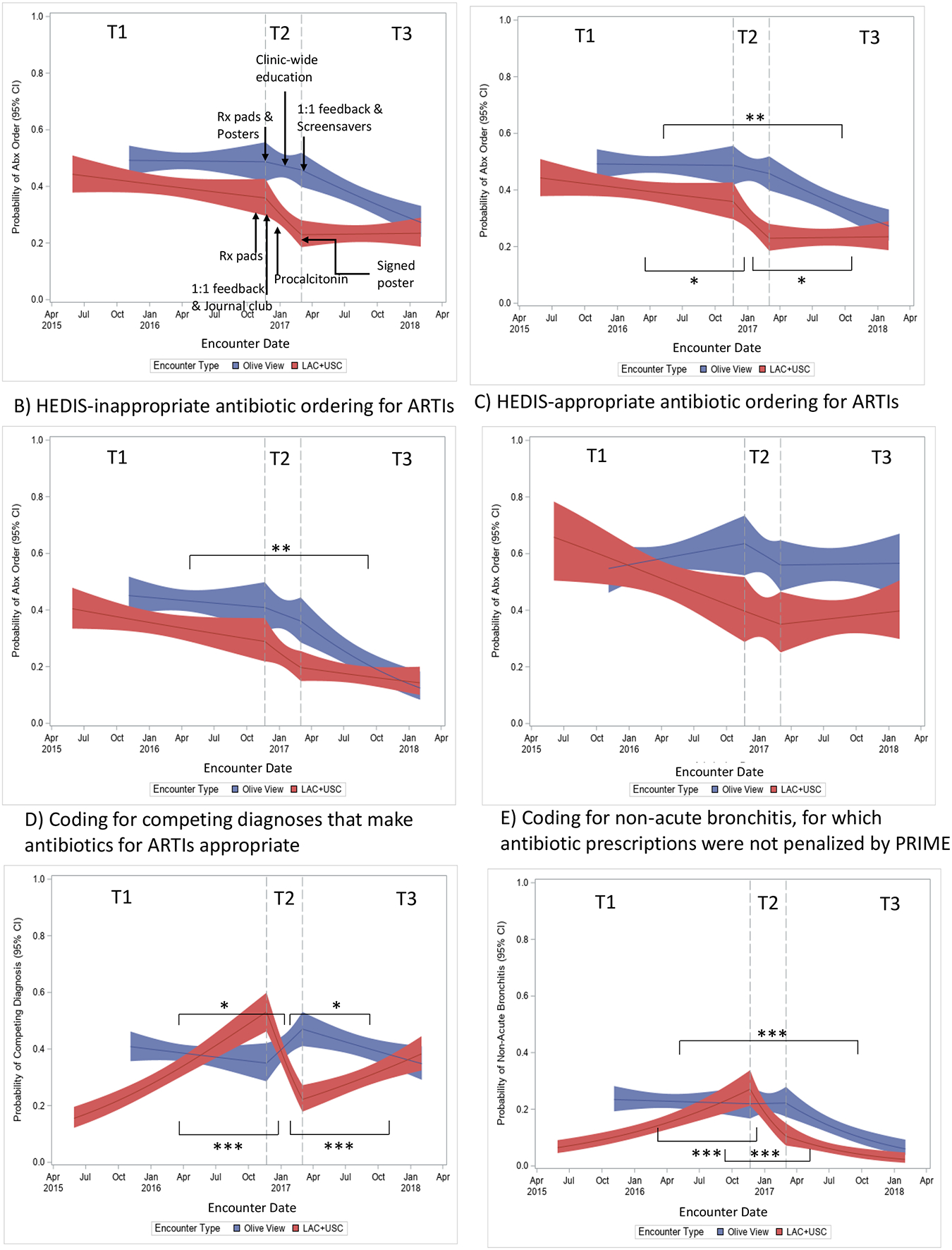
Methods: A nonrandomized intervention (5/28/2015-2/1/2018) was conducted at 2 large academic safety-net hospitals: Los Angeles County+University of Southern California (LAC+USC) and Olive View-UCLA (OV-UCLA). In response to California's 2016 P4P program to reduce antibiotics for acute bronchitis, 5 staggered Choosing Wisely-based interventions were launched in combination: audit and feedback, clinician education, suggested alternatives, procalcitonin, and public commitment. We also assessed 5 unintended effects: reductions in Healthcare Effectiveness Data and Information Set (HEDIS)-appropriate prescribing, diagnosis shifting, substituting antibiotics with steroids, increasing antibiotics for ARTIs not penalized by the P4P program, and inappropriate withholding of antibiotics.
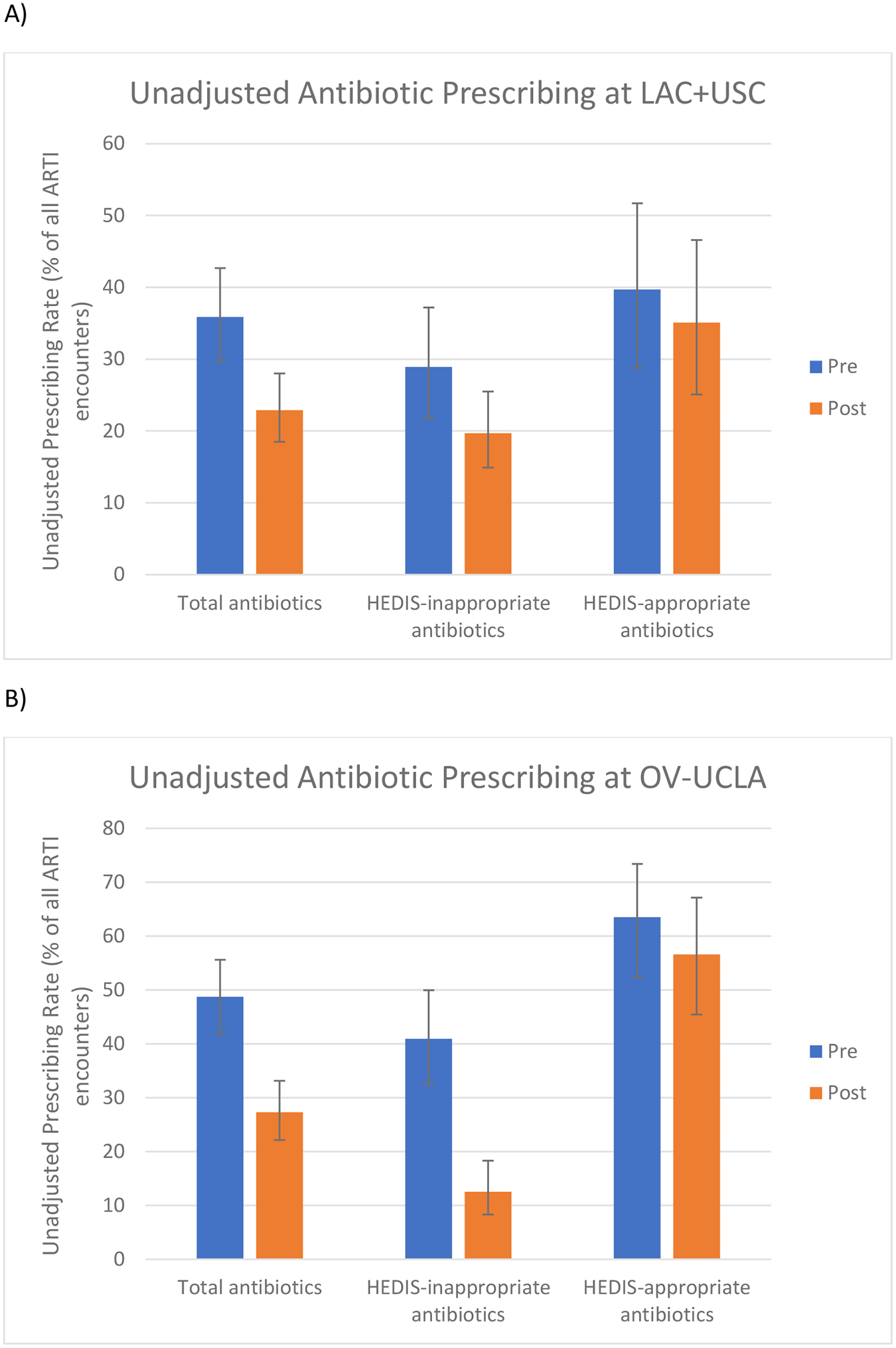
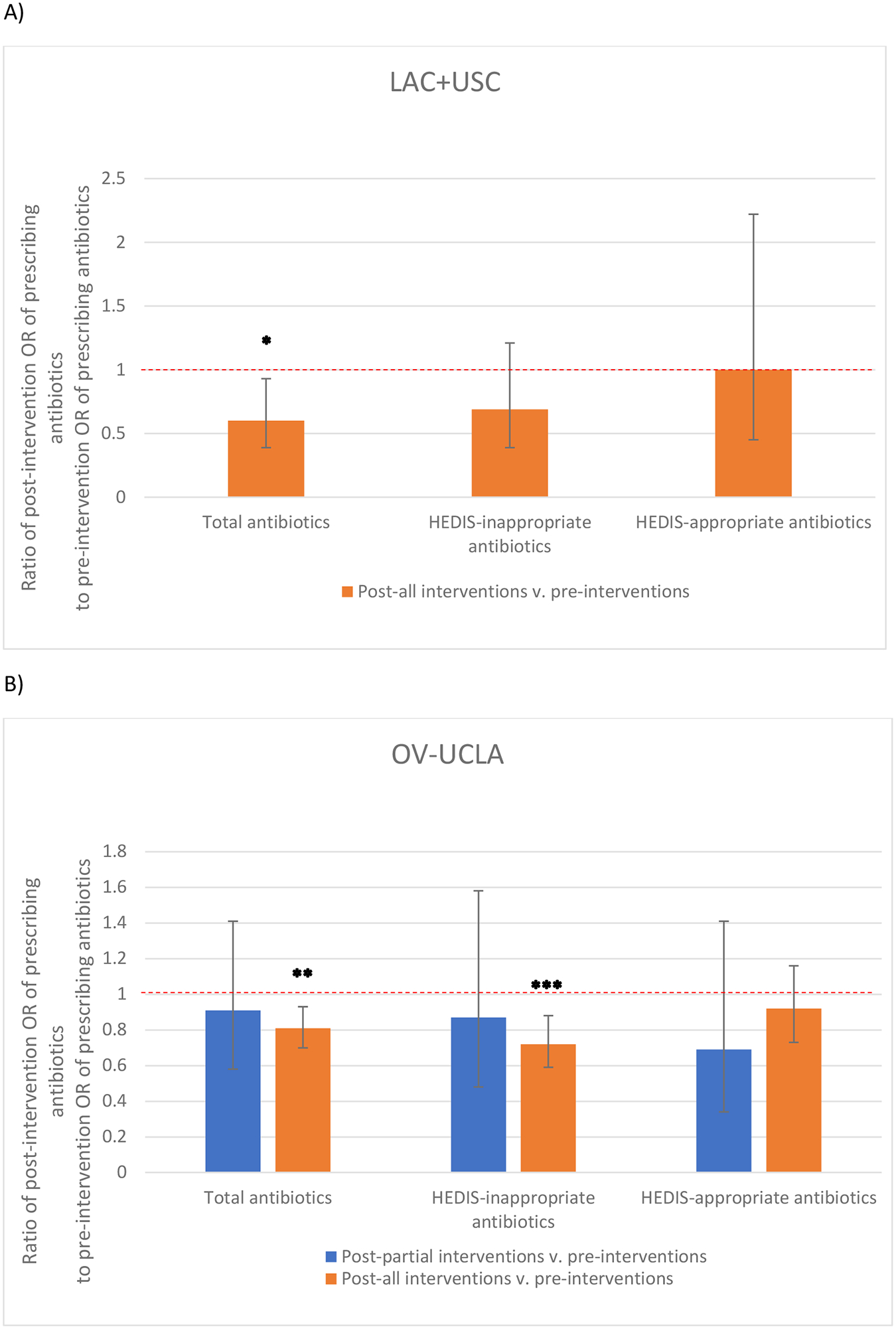
Results: Among 3583 consecutive patients with ARTIs, mean antibiotic prescribing rates for ARTIs decreased from 35.9% to 22.9% (odds ratio [OR], 0.60; 95% CI, 0.39-0.93) at LAC+USC and from 48.7% to 27.3% (OR, 0.81; 95% CI, 0.70-0.93) at OV-UCLA after the intervention. HEDIS-inappropriate prescribing rates decreased from 28.9% to 19.7% (OR, 0.69; 95% CI, 0.39-1.21) at LAC+USC and from 40.9% to 12.5% (OR, 0.72; 95% CI, 0.59-0.88) at OV-UCLA. There was no evidence of unintended consequences.
Conclusions: These real-world multicomponent interventions responding to P4P incentives were associated with substantial reductions in antibiotic prescriptions for ARTIs in 2 safety-net health systems without unintended harms.
Figures