

The stroke transitional care intervention for older adults with stroke and multimorbidity: a multisite pragmatic randomized controlled trial
- PMID: 37872479
- PMCID: PMC10594728
- DOI: 10.1186/s12877-023-04403-1
The stroke transitional care intervention for older adults with stroke and multimorbidity: a multisite pragmatic randomized controlled trial
Abstract
Background: This study aimed to test, in real-world clinical practice, the effectiveness of a Transitional Care Stroke Intervention (TCSI) compared to usual care on health outcomes, self-management, patient experience, and health and social service use costs in older adults (≥ 55 years) with stroke and multimorbidity (≥ 2 chronic conditions).
Methods: This pragmatic randomized controlled trial (RCT) included older adults discharged from hospital to community with stroke and multimorbidity using outpatient stroke rehabilitation services in two communities in Ontario, Canada. Participants were randomized 1:1 to usual care (control group) or usual care plus the 6-month TCSI (intervention group). The TCSI was delivered virtually by an interprofessional (IP) team, and included care coordination/system navigation support, phone/video visits, monthly IP team conferences, and an online resource to support system navigation. The primary outcome was risk of hospital readmission (all cause) after six-months. Secondary outcomes included physical and mental functioning, stroke self-management, patient experience, and health and social service use costs. The intention-to-treat principle was used to conduct the primary and secondary analyses.
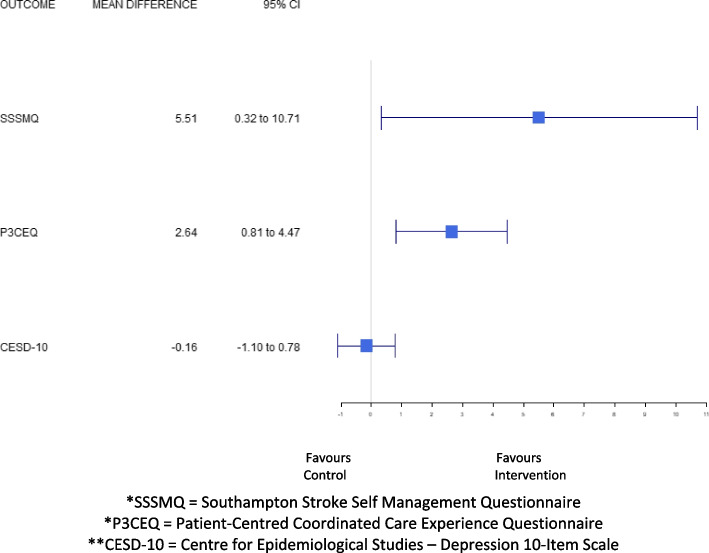
Results: Ninety participants were enrolled (44 intervention, 46 control); 11 (12%) participants were lost to follow-up, leaving 79 (39 intervention, 40 control). No significant between-group differences were seen for baseline to six-month risk of hospital readmission. Differences favouring the intervention group were seen in the following secondary outcomes: physical functioning (SF-12 PCS mean difference: 5.10; 95% CI: 1.58-8.62, p = 0.005), stroke self-management (Southampton Stroke Self-Management Questionnaire mean difference: 6.00; 95% CI: 0.51-11.50, p = 0.03), and patient experience (Person-Centred Coordinated Care Experiences Questionnaire mean difference: 2.64, 95% CI: 0.81, 4.47, p = 0.005). No between-group differences were found in total healthcare costs or other secondary outcomes.
Conclusions: Although participation in the TCSI did not impact hospital readmissions, there were improvements in physical functioning, stroke self-management and patient experience in older adults with stroke and multimorbidity without increasing total healthcare costs. Challenges associated with the COVID-19 pandemic, including the shift from in-person to virtual delivery, and re-deployment of interventionists could have influenced the results. A larger pragmatic RCT is needed to determine intervention effectiveness in diverse geographic settings and ethno-cultural populations and examine intervention scalability.
Trial registration: ClinicalTrials.gov Identifier: NCT04278794 . Registered May 2, 2020.
Keywords: Community-based care; Costs; Effectiveness; Healthcare intervention; Multimorbidity; Older adults; Stroke rehabilitation; Transitions.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Canada Go . Stroke in Canada: Highlights from the Canadian Chronic Disease Surveillance System. 2023.
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344–e418. doi: 10.1161/STR.0000000000000211. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
