

State-Level Adverse Outcomes Among Long-Term Services and Supports Users With Alzheimer's Disease and Related Dementias
- PMID: 37872791
- PMCID: PMC12176509
- DOI: 10.1177/10775587231207668
State-Level Adverse Outcomes Among Long-Term Services and Supports Users With Alzheimer's Disease and Related Dementias
Abstract
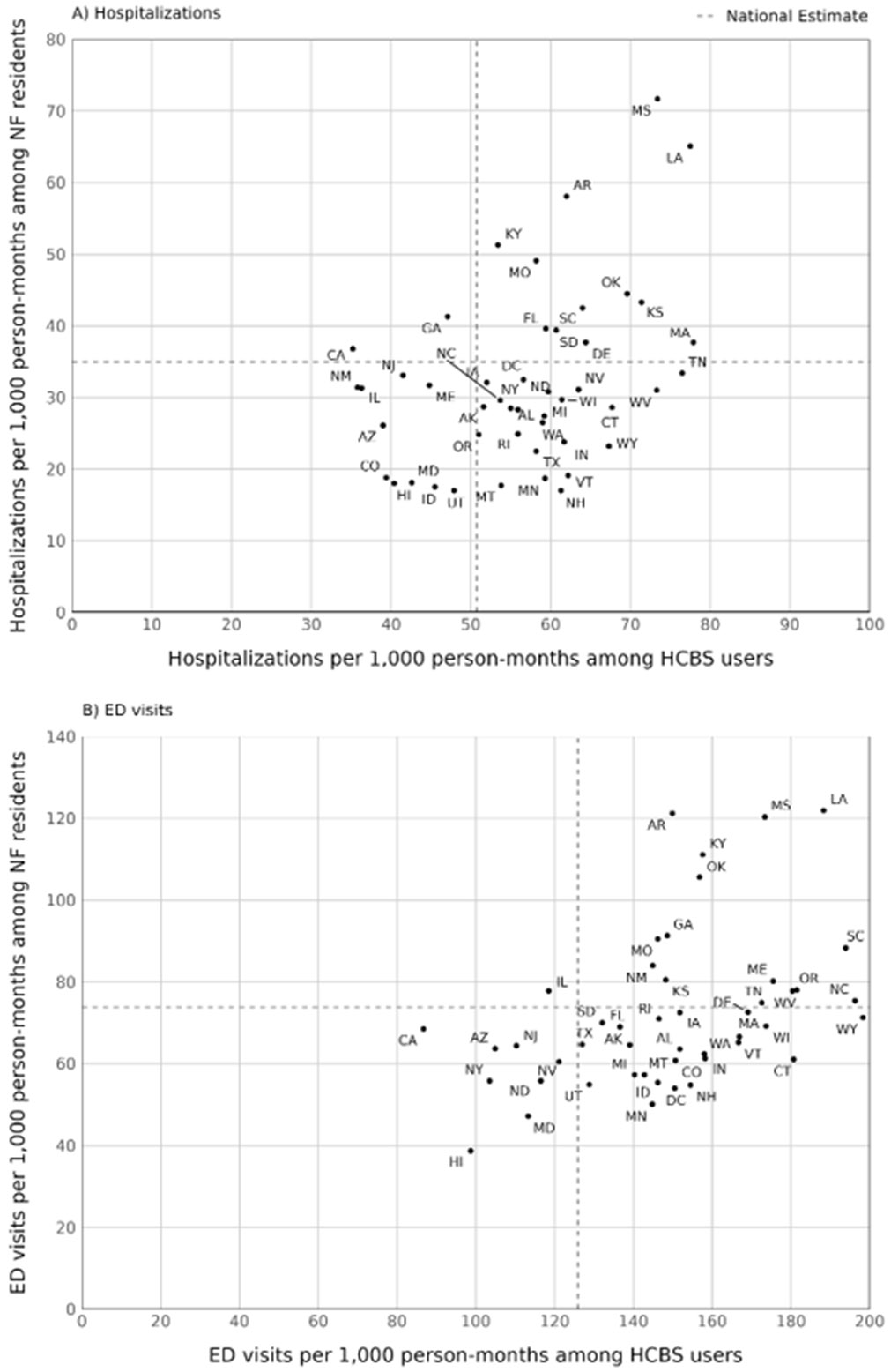
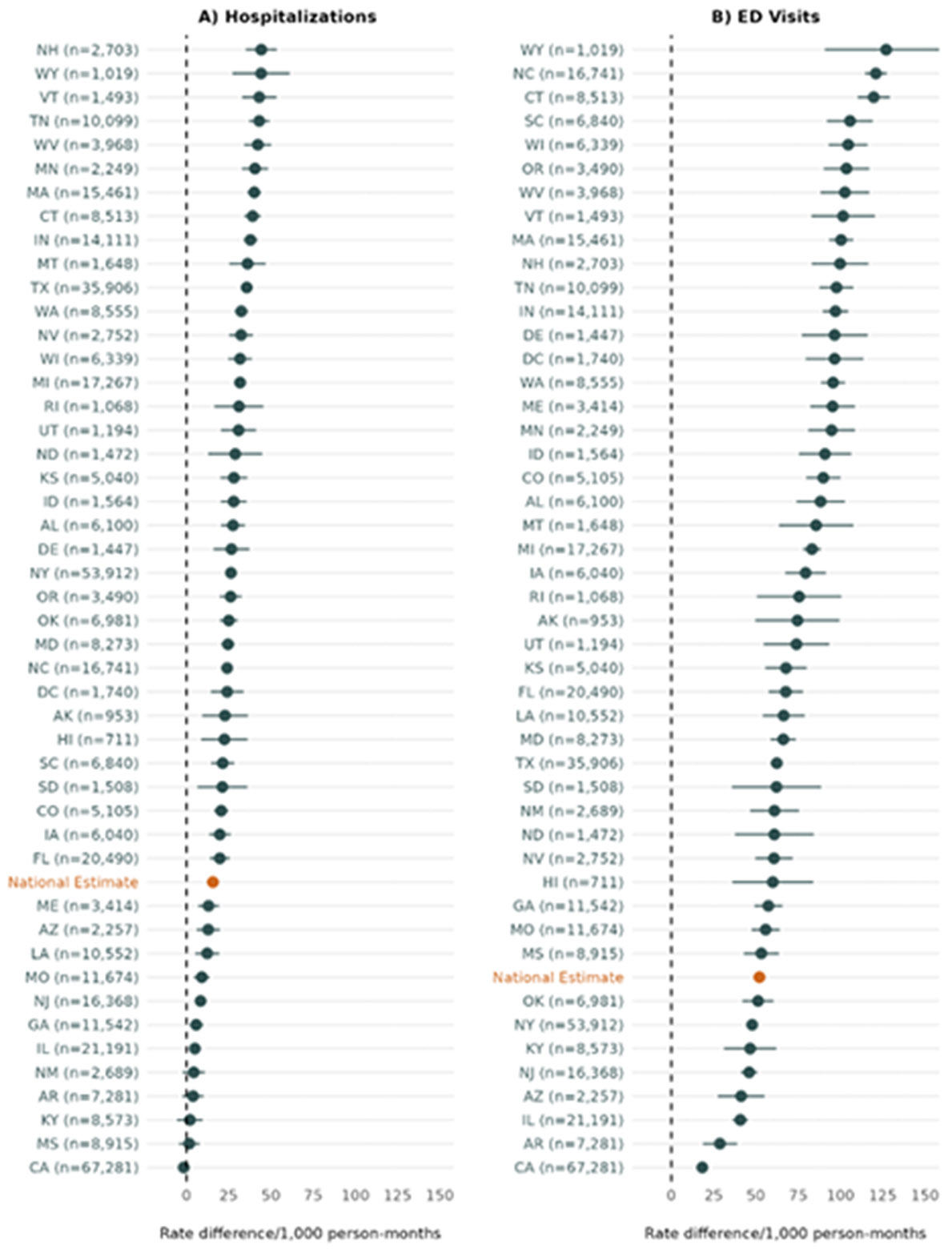
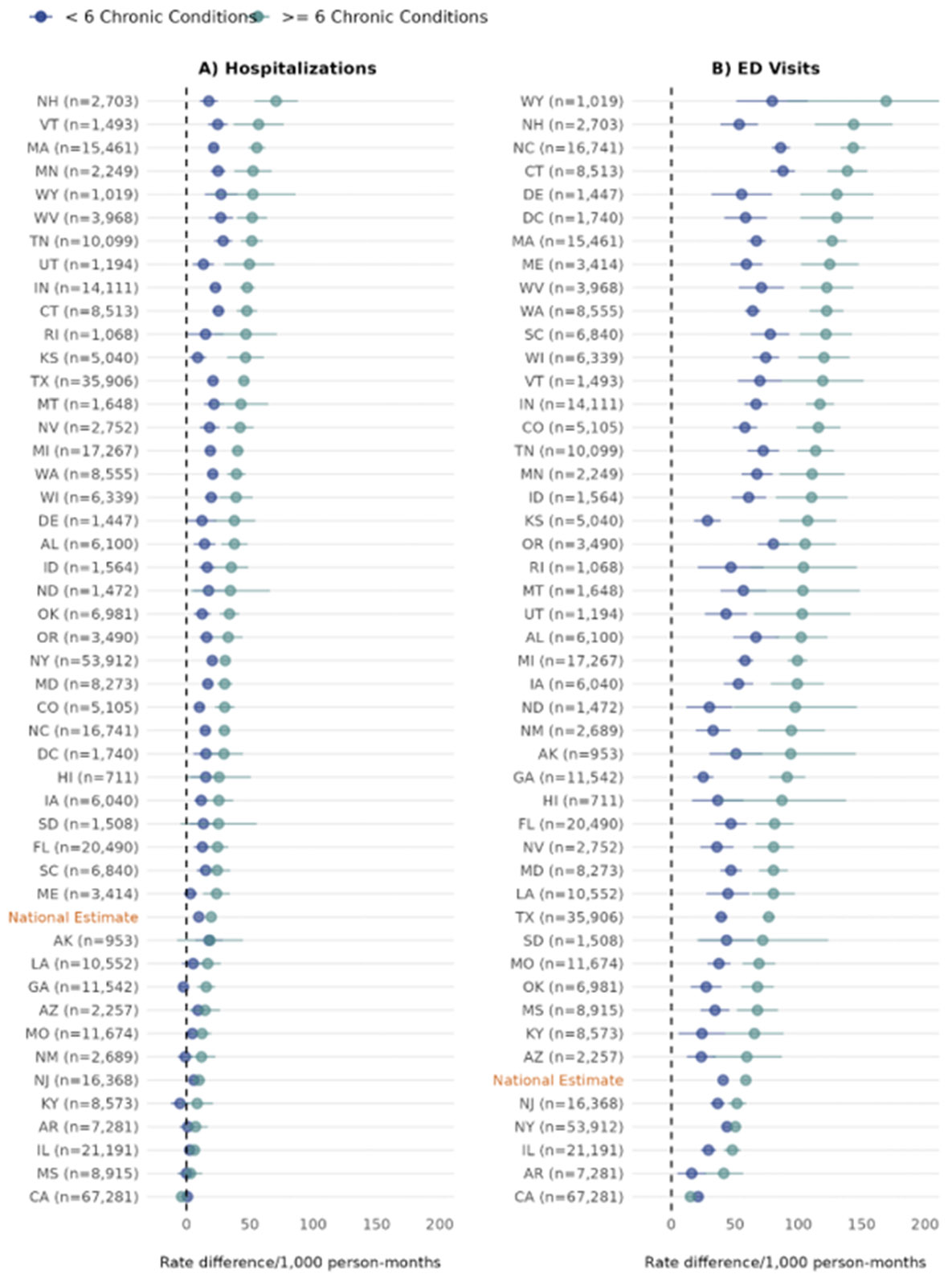
Home- and community-based services (HCBS) users, on average, experience hospitalizations more frequently than nursing facility residents. However, little is known about state-level variation in such adverse events among these groups. Using 2018 Medicare and Medicaid claims for dual-eligible beneficiaries with Alzheimer's disease and related dementias, we described hospitalization and emergency department (ED) visit rates among HCBS users and nursing facility residents and observed substantial state-level variation. In addition, consistent with prior evidence, we found more frequent hospitalizations and ED visits among HCBS users than nursing facility residents. The magnitude of this difference varied considerably across states, and the degree of variation was greatest among beneficiaries with six or more comorbid conditions. Our findings represent a crucial initial exploration of the state-level variation in adverse events among HCBS users and nursing facility residents, paving the way for further investigations into factors that contribute to this variability.
Keywords: LTSS; dementia; dual-eligibles.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Alzheimer’s Association. (2022). Factsheet: Medicaid and seniors with Alzheimer’s. https://alzimpact.org/media/serve/id/5ab115bad5065
-
- American Council on Aging. (2021, February 17). What is Nursing Home Level of Care & Its Importance to Medicaid Eligibility. https://www.medicaidplanningassistance.org/nursing-home-level-of-care/
-
- Chronic Conditions Data Warehouse. (2019). Condition Categories. https://www.ccwdata.org/web/guest/condition-categories
-
- Chronic Conditions Data Warehouse. (2023). Condition Categories. https://www2.ccwdata.org/web/guest/condition-categories
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
