

Atypical ductal hyperplasia on vacuum-assisted breast biopsy: a scoring system to predict the risk of upgrade to malignancy
- PMID: 37874442
- PMCID: PMC10808485
- DOI: 10.1007/s11547-023-01740-4
Atypical ductal hyperplasia on vacuum-assisted breast biopsy: a scoring system to predict the risk of upgrade to malignancy
Abstract
Rationale and objectives: Our multicentric study analysed clinical, radiologic and pathologic features in patients with atypical ductal hyperplasia (ADH) diagnosed with vacuum-assisted biopsy (VAB), to identify factors associated with the risk of upgrade, to develop a scoring system to support decision making.
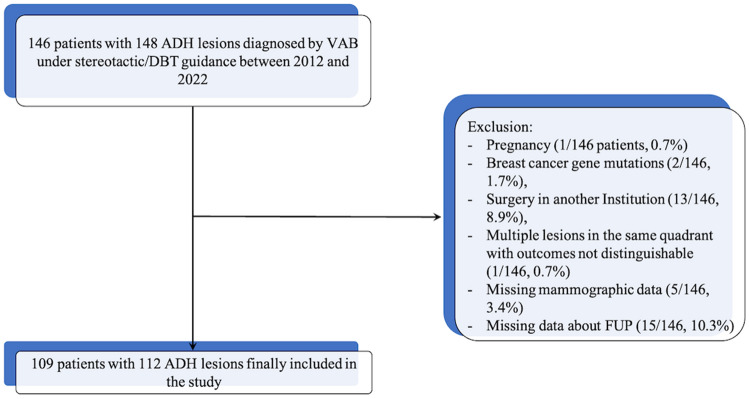
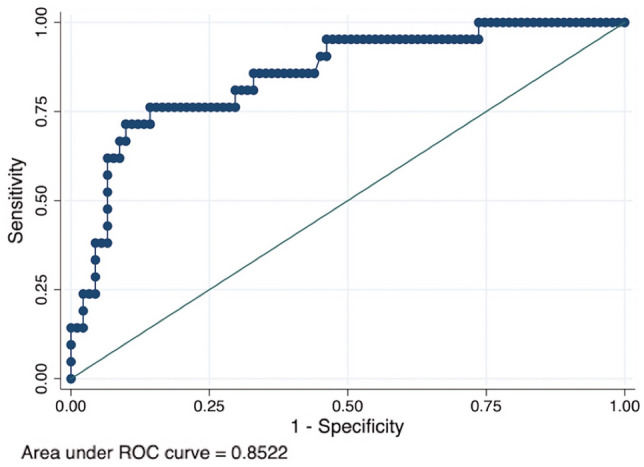
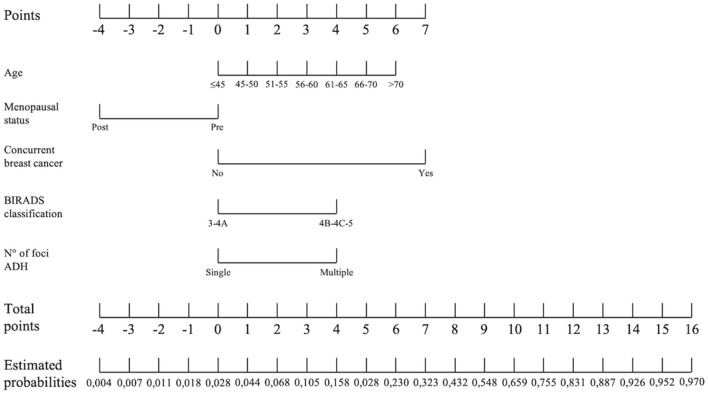
Materials and methods: Patients with ADH on VAB under stereotactic/tomosynthesis guidance (2012-2022) were eligible. Inclusion criteria were availability of surgical histopathological examination of the entire lesion or radiologic follow-up (FUP) ≥ 24 months. VAB results were compared with surgical pathological results or with imaging FUP evolution to assess upgrade. A backward stepwise linear regression was used to identify predictors of upgrade. The discriminatory power of the model was calculated through the area under the receiver operating curve (ROC-AUC); the Hosmer-Lemeshow test was used to assess model calibration. The points system was developed based on the selected risk factors, and the probability of upgrade associated with each point total was determined.
Results: 112 ADH lesions were included: 91 (91/112, 81.3%) underwent surgical excision with 20 diagnosis of malignancy, while 21 (21/112, 18.7%) underwent imaging FUP with one interval change (mean FUP time 48 months). Overall upgrade rate was 18.7% (21/112). Age, menopausal status, concurrent breast cancer, BIRADS classification and number of foci of ADH were identified as risk factors for upgrade. Our model showed an AUC = 0.85 (95% CI 0.76-0.94). The points system showed that the risk of upgrade is < 2% when the total score is ≤ 1.
Conclusion: Our scoring system seemed a promising easy-to-use decision support tool for management of ADH, decreasing unnecessary surgeries, reducing patients' overtreatment and healthcare costs.
Keywords: Atypical ductal hyperplasia; Scoring system; Underestimation; Upgrade; Vacuum-assisted biopsy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Tavassoli FA (1999) Pathology of the Breast. Stamford, CT: Appleton & Lange
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
