

Screening uptake of colonoscopy versus fecal immunochemical testing in first-degree relatives of patients with non-syndromic colorectal cancer: A multicenter, open-label, parallel-group, randomized trial (ParCoFit study)
- PMID: 37874831
- PMCID: PMC10597530
- DOI: 10.1371/journal.pmed.1004298
Screening uptake of colonoscopy versus fecal immunochemical testing in first-degree relatives of patients with non-syndromic colorectal cancer: A multicenter, open-label, parallel-group, randomized trial (ParCoFit study)
Abstract
Background: Colonoscopy screening is underused by first-degree relatives (FDRs) of patients with non-syndromic colorectal cancer (CRC) with screening completion rates below 50%. Studies conducted in FDR referred for screening suggest that fecal immunochemical testing (FIT) was not inferior to colonoscopy in terms of diagnostic yield and tumor staging, but screening uptake of FIT has not yet been tested in this population. In this study, we investigated whether the uptake of FIT screening is superior to the uptake of colonoscopy screening in the familial-risk population, with an equivalent effect on CRC detection.
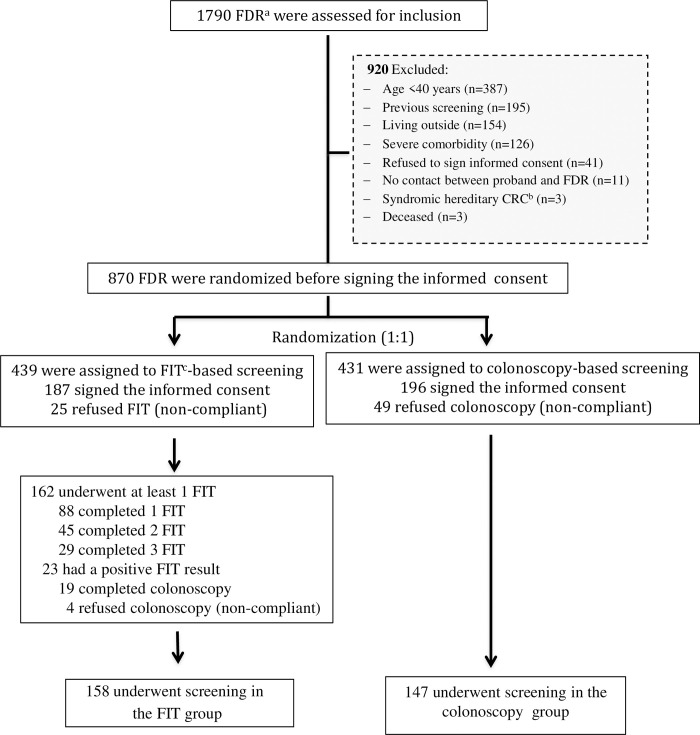
Methods and findings: This open-label, parallel-group, randomized trial was conducted in 12 Spanish centers between February 2016 and December 2021. Eligible individuals included asymptomatic FDR of index cases <60 years, siblings or ≥2 FDR with CRC. The primary outcome was to compare screening uptake between colonoscopy and FIT. The secondary outcome was to determine the efficacy of each strategy to detect advanced colorectal neoplasia (adenoma or serrated polyps ≥10 mm, polyps with tubulovillous architecture, high-grade dysplasia, and/or CRC). Screening-naïve FDR were randomized (1:1) to one-time colonoscopy versus annual FIT during 3 consecutive years followed by a work-up colonoscopy in the case of a positive test. Randomization was performed before signing the informed consent using computer-generated allocation algorithm based on stratified block randomization. Multivariable regression analysis was performed by intention-to-screen. On December 31, 2019, when 81% of the estimated sample size was reached, the trial was terminated prematurely after an interim analysis for futility. Study outcomes were further analyzed through 2-year follow-up. The main limitation of this study was the impossibility of collecting information on eligible individuals who declined to participate. A total of 1,790 FDR of 460 index cases were evaluated for inclusion, of whom 870 were assigned to undergo one-time colonoscopy (n = 431) or FIT (n = 439). Of them, 383 (44.0%) attended the appointment and signed the informed consent: 147/431 (34.1%) FDR received colonoscopy-based screening and 158/439 (35.9%) underwent FIT-based screening (odds ratio [OR] 1.08; 95% confidence intervals [CI] [0.82, 1.44], p = 0.564). The detection rate of advanced colorectal neoplasia was significantly higher in the colonoscopy group than in the FIT group (OR 3.64, 95% CI [1.55, 8.53], p = 0.003). Study outcomes did not change throughout follow-up.
Conclusions: In this study, compared to colonoscopy, FIT screening did not improve screening uptake by individuals at high risk of CRC, resulting in less detection of advanced colorectal neoplasia. Further studies are needed to assess how screening uptake could be improved in this high-risk group, including by inclusion in population-based screening programs.
Trial registration: This trial was registered with ClinicalTrials.gov (NCT02567045).
Copyright: © 2023 González-López et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
EQ and AL received an honorarium for consultancy from Sysmex (2017–2020). FB received endoscopic equipment on loan of Fujifilm, received an honorarium for consultancy from Sysmex (2017–2020) and editorial fee from Elsevier as editor of Gastroenterologia y Hepatologia. The other authors declare no conflict of interest regarding this study.
Figures
References
-
- Monahan KJ, Bradshaw N, Dolwani S, Desouza B, Dunlop MG, East JE, et al. Guidelines for the management of hereditary colorectal cancer from the British Society of Gastroenterology (BSG)/Association of Coloproctology of Great Britain and Ireland (ACPGBI)/United Kingdom Cancer Genetics Group (UKCGG). Gut. 2020;69 (3):411–444. doi: 10.1136/gutjnl-2019-319915 . - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
