

Potential role for extracorporeal membrane oxygenation cardiopulmonary resuscitation (E-CPR) during in-hospital cardiac arrest in Australia: A nested cohort study
- PMID: 37876603
- PMCID: PMC10581279
- DOI: 10.1016/j.ccrj.2023.05.006
Potential role for extracorporeal membrane oxygenation cardiopulmonary resuscitation (E-CPR) during in-hospital cardiac arrest in Australia: A nested cohort study
Erratum in
-
Erratum for previously published articles.Crit Care Resusc. 2023 Oct 12;25(3):158. doi: 10.1016/j.ccrj.2023.09.001. eCollection 2023 Sep. Crit Care Resusc. 2023. PMID: 39726436 Free PMC article.
Abstract
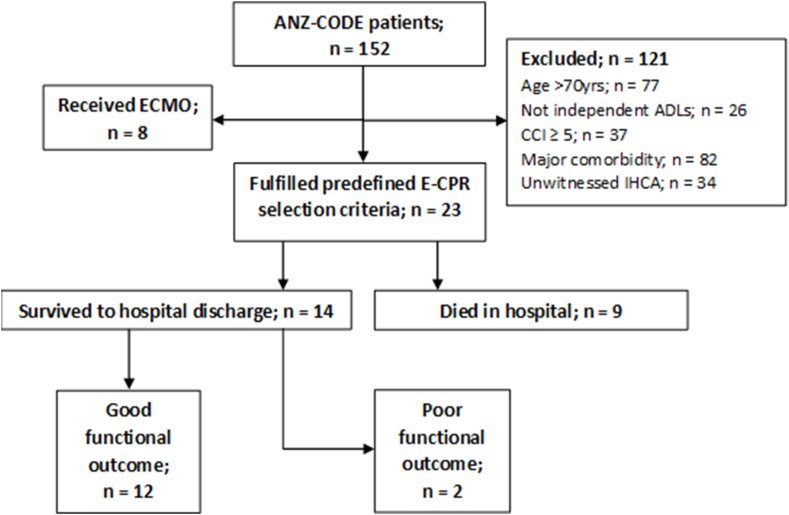
Objective: This study aims to evaluate the characteristics and outcomes of patients who fulfilled extracorporeal membrane oxygenation cardiopulmonary resuscitation (E-CPR) selection criteria during in-hospital cardiac arrest (IHCA).
Design: This is a nested cohort study.
Setting: Code blue data were collected across seven hospitals in Australia between July 2017 and August 2018.
Participants: Participants who fulfilled E-CPR selection criteria during IHCA were included.
Main outcome measures: Return of spontaneous circulation and survival and functional outcome at hospital discharge. Functional outcome was measured using the modified Rankin scale, with scores dichotomised into good and poor functional outcome.
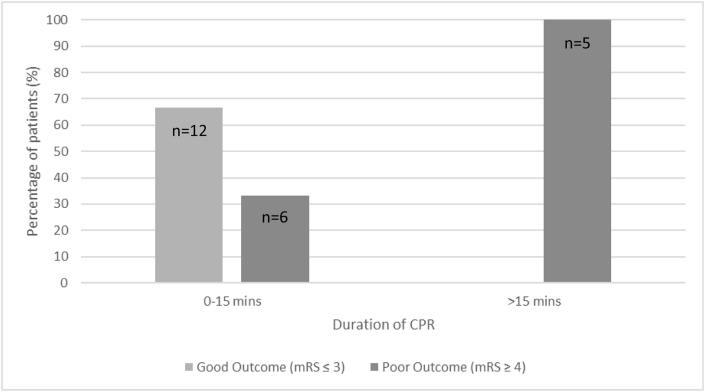
Results: Twenty-three (23/144; 16%) patients fulfilled E-CPR selection criteria during IHCA, and 11/23 (47.8%) had a poor outcome. Patients with a poor outcome were more likely to have a non-shockable rhythm (81.8% vs. 16.7%; p = 0.002), and a longer duration of CPR (median 12.5 [5.5, 39.5] vs. 1.5 [0.3, 2.5] minutes; p < 0.001) compared to those with a good outcome. The majority of patients (18/19 [94.7%]) achieved sustained return of spontaneous circulation within 15 minutes of CPR. All five patients who had CPR >15 minutes had a poor outcome.
Conclusion: Approximately one in six IHCA patients fulfilled E-CPR selection criteria during IHCA, half of whom had a poor outcome. Non-shockable rhythm and longer duration of CPR were associated with poor outcome. Patients who had CPR for >15 minutes and a poor outcome may have benefited from E-CPR. The feasibility, effectiveness and risks of commencing E-CPR earlier in IHCA and among those with non-shockable rhythms requires further investigation.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation; Extracorporeal membrane oxygenation; Intensive care.
© 2023 The Authors.
Figures
References
-
- Straney L.D., Bray J.E., Finn J., Bernard S. Trends in intensive care unit cardiac arrest admissions and mortality in Australia and New Zealand. Crit Care Resusc. 2014;16(2):104–111. - PubMed
-
- Nolan J.P., Soar J., Smith G.B., Gwinnutt C., Parrott F., Power S., et al. Incidence and outcome of in-hospital cardiac arrest in the United Kingdom national cardiac arrest audit. Resuscitation. 2014;85(8):987–992. - PubMed
LinkOut - more resources
Full Text Sources
