

Immunotherapy and brain metastasis in lung cancer: connecting bench side science to the clinic
- PMID: 37876939
- PMCID: PMC10590916
- DOI: 10.3389/fimmu.2023.1221097
Immunotherapy and brain metastasis in lung cancer: connecting bench side science to the clinic
Abstract
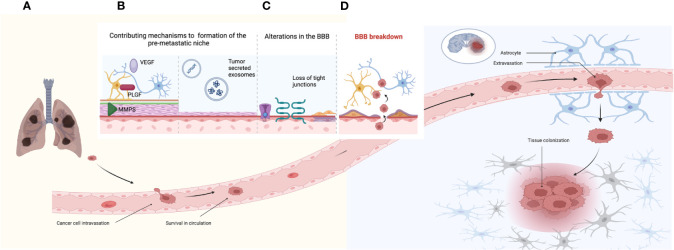
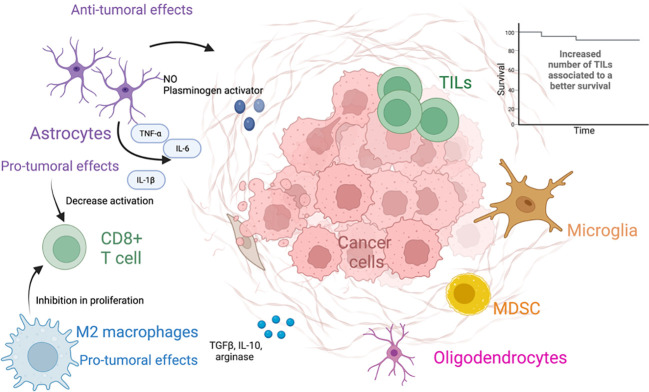
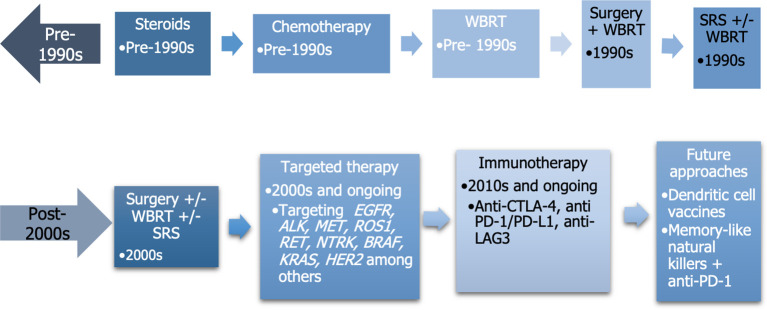
Brain metastases (BMs) are the most common form of intracranial malignant neoplasms in adults, with a profound impact on quality of life and traditionally associated with a dismal prognosis. Lung cancer accounts for approximately 40%-50% of BM across different tumors. The process leading to BMs is complex and includes local invasion, intravasation, tumor cells circulation into the bloodstream, disruption of the blood-brain barrier, extravasation of tumor cells into the brain parenchyma, and interaction with cells of the brain microenvironment, among others. Once the tumor cells have seeded in the brain parenchyma, they encounter different glial cells of the brain, as well as immune cells. The interaction between these cells and tumor cells is complex and is associated with both antitumoral and protumoral effects. To overcome the lethal prognosis associated with BMs, different treatment strategies have been developed, such as immunotherapy with immune checkpoint inhibitors, particularly inhibitors of the PD-1/PD-L1 axis, which have demonstrated to be an effective treatment in both non-small cell lung cancer and small cell lung cancer. These antibodies have shown to be effective in the treatment of BM, alone or in combination with chemotherapy or radiotherapy. However, many unsolved questions remain to be answered, such as the sequencing of immunotherapy and radiotherapy, the optimal management in symptomatic BMs, the role of the addition of anti-CTLA-4 antibodies, and so forth. The complexity in the management of BMs in the era of immunotherapy requires a multidisciplinary approach to adequately treat this devastating event. The aim of this review is to summarize evidence regarding epidemiology of BM, its pathophysiology, current approach to treatment strategies, as well as future perspectives.
Keywords: NSCLC; SCLC; brain metastases; immune microenvironment; immunotherapy.
Copyright © 2023 Rios-Hoyo and Arriola.
Conflict of interest statement
EA reports the following COIs: Consulting or Advisory Role: MSD, Bristol-Myers, Roche, Boehringer Ingelheim, Pfizer, Novartis, AstraZeneca, Lilly, Takeda. Speaking: MSD, Bristol-Myers, Roche, Boehringer Ingelheim, Pfizer, Novartis, AstraZeneca, Lilly, Takeda. Co-founder: Trialing Health S.L. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials