

Cutaneous T-cell lymphoma with CNS involvement: a case series and review of the literature
- PMID: 37877303
- PMCID: PMC10701703
- DOI: 10.2217/cns-2023-0014
Cutaneous T-cell lymphoma with CNS involvement: a case series and review of the literature
Abstract
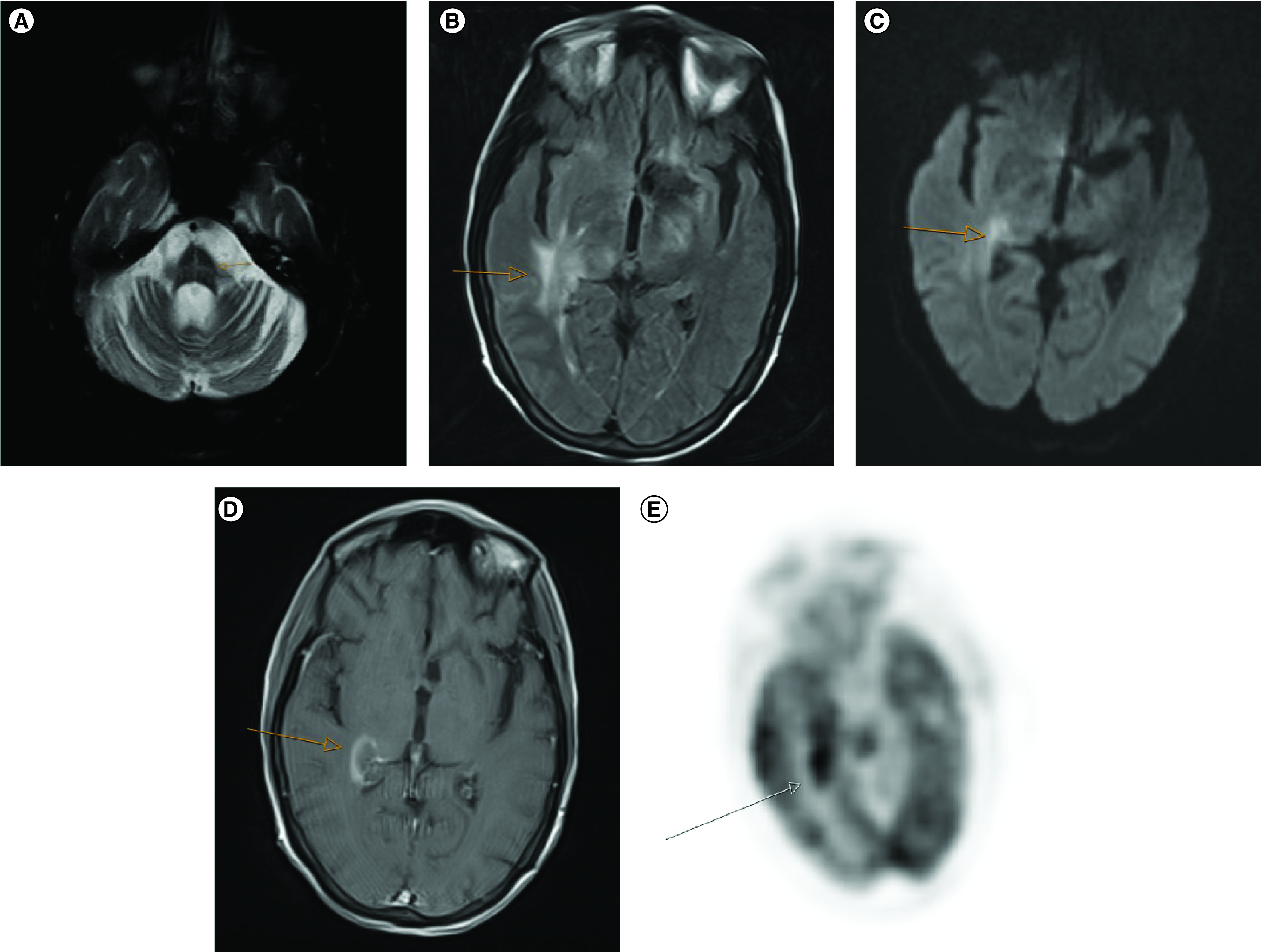
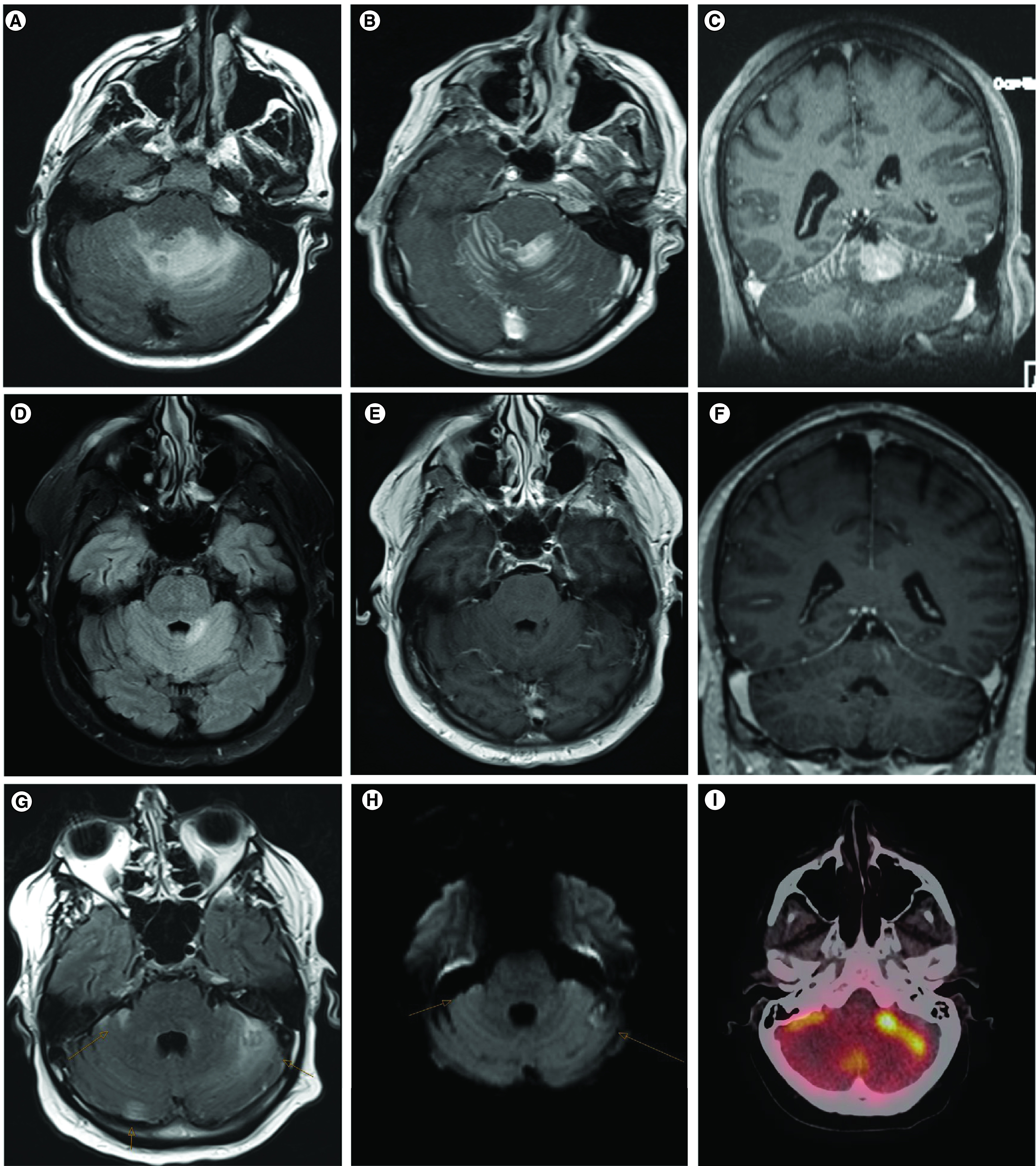
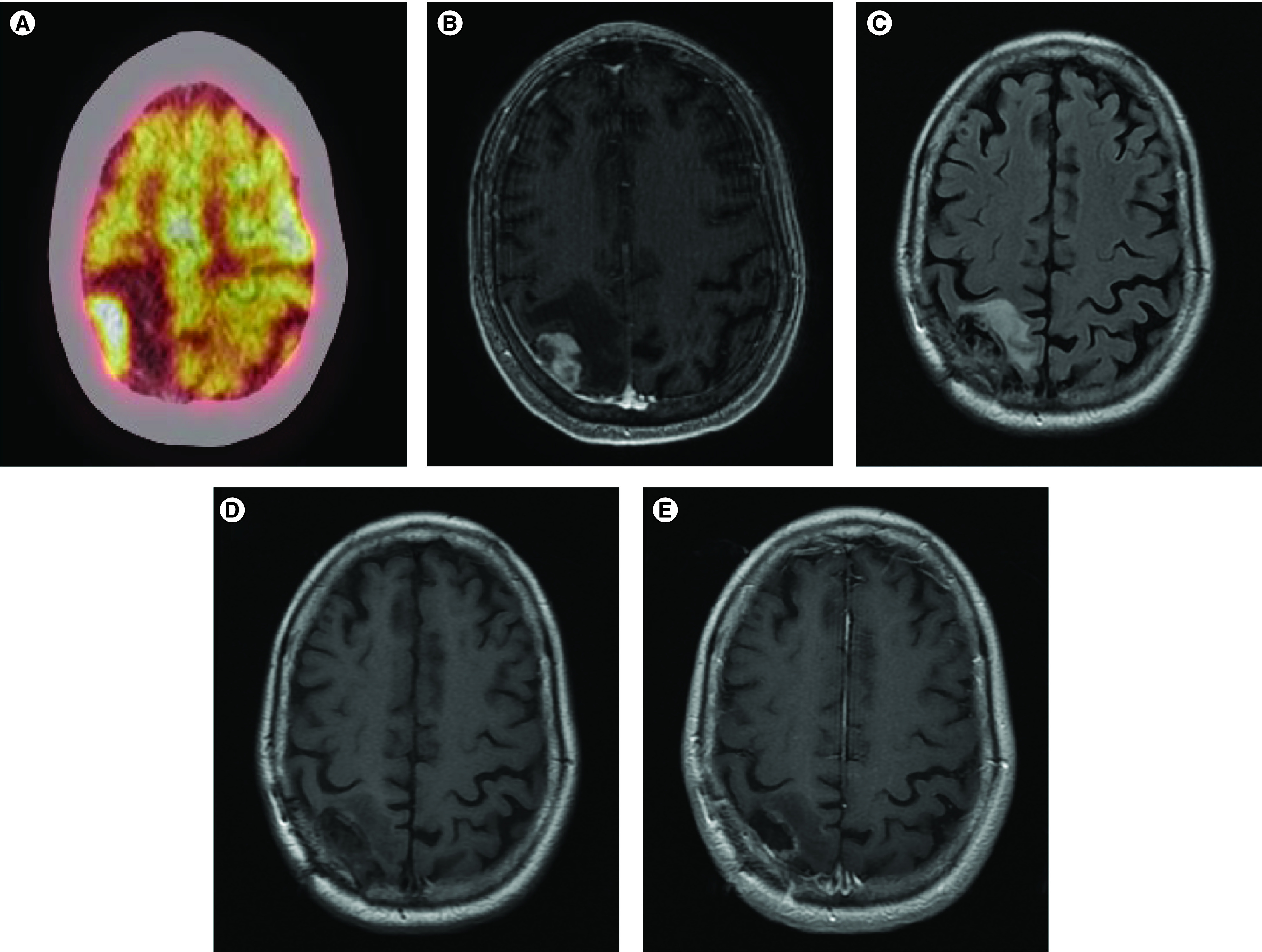
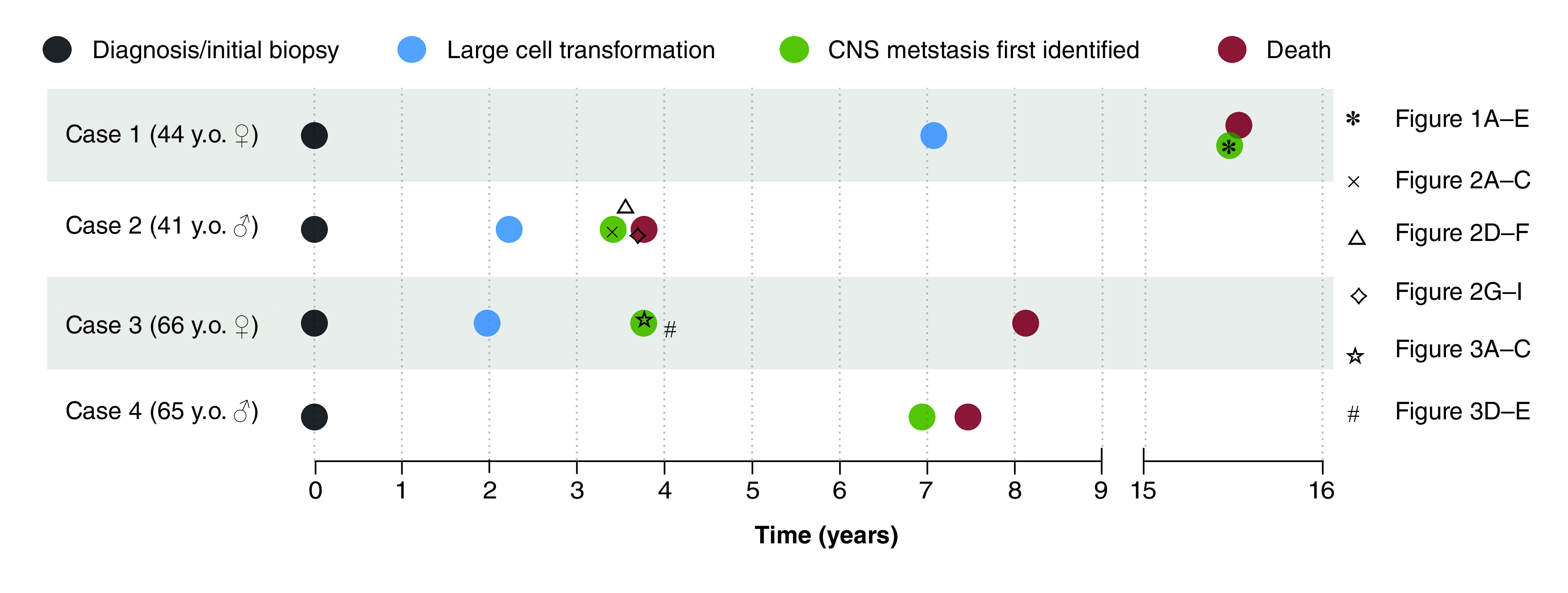
Cutaneous T-cell lymphoma (CTCL) is a rare hematologic malignancy that traditionally presents with cutaneous lesions, though metastases are not uncommon in progressive disease. We describe four cases of CTCL with central nervous system (CNS) involvement, detailing the history, pathological characteristics, treatment response, and progression. Median time from initial diagnosis to CNS metastasis was ∼5.4 years (range 3.4-15.5 years) and survival after metastasis was ∼160 days (range 19 days-4.4 years). No patients achieved long-term (>5 years) survival, though some displayed varying degrees of remission following CNS-directed therapy. We conclude that clinicians must be attentive to the development of CNS metastases in patients with CTCL. The growing body of literature on such cases will inform evolving therapeutic guidelines on this rare CTCL complication.
Keywords: Sezary syndrome; brain; metastasis; mycosis fungoides; visceral.
Plain language summary
Cutaneous T-cell lymphoma (CTCL) is a rare cancer of the blood, which typically manifests with skin lesions, such as itchy, scaly rashes that may thicken to form tumors on the skin. Though uncommon, metastases do occur in CTCL. A particularly rare location for these metastases is the central nervous system. This case series recounts the story of four unique patients and the presentation, diagnosis, and treatment of their CTCL, which unfortunately progressed to involve the central nervous system. Outcomes with central nervous system involvement in CTCL are poor, but may occur sometime later than a patient's initial diagnosis. Our patients had a median time from initial diagnosis to central nervous system metastases of ∼5.4 years and a survival of ∼160 days after central nervous system metastases. Some types of therapy, such as radiation, surgery, or chemotherapy, may be beneficial in extending survival or providing symptomatic relief for patients. It can be difficult to recognize symptoms of central nervous system metastases, so this case series emphasizes that vigilance for potential metastases and use of interdisciplinary teams is important in caring for these patients. This case series demonstrates the importance of continued research in this area, with the hope of improving outcomes for patients with central nervous system metastases of CTCL.
Conflict of interest statement
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Figures
Similar articles
-
Extracorporeal photophoresis: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(6):1-82. Epub 2006 Mar 1. Ont Health Technol Assess Ser. 2006. PMID: 23074497 Free PMC article.
-
Cutaneous T cell lymphoma in children.Semin Cutan Med Surg. 1999 Sep;18(3):226-32. doi: 10.1016/s1085-5629(99)80020-0. Semin Cutan Med Surg. 1999. PMID: 10468042 Review.
-
Overall survival in erythrodermic cutaneous T-cell lymphoma: an analysis of prognostic factors in a cohort of patients with erythrodermic cutaneous T-cell lymphoma.Int J Dermatol. 2009 Mar;48(3):243-52. doi: 10.1111/j.1365-4632.2009.03771.x. Int J Dermatol. 2009. PMID: 19261011
-
Cutaneous gamma-delta T-cell lymphoma with central nervous system involvement: report of a rarity with review of literature.J Cutan Pathol. 2014 Dec;41(12):936-43. doi: 10.1111/cup.12395. Epub 2014 Nov 11. J Cutan Pathol. 2014. PMID: 25292289 Review.
-
Clinicopathologic Features of Cutaneous T-Cell Lymphomas With Extracutaneous Metastasis: A Case Series.Clin Lymphoma Myeloma Leuk. 2023 Nov;23(11):e405-e410. doi: 10.1016/j.clml.2023.08.006. Epub 2023 Aug 14. Clin Lymphoma Myeloma Leuk. 2023. PMID: 37659965
Cited by
-
A comprehensive update of extracutaneous involvement of mycosis fungoides: A narrative review of literature.Medicine (Baltimore). 2025 May 9;104(19):e42279. doi: 10.1097/MD.0000000000042279. Medicine (Baltimore). 2025. PMID: 40355202 Free PMC article. Review.
References
-
- Dummer R, Vermeer MH, Scarisbrick JJ et al. Cutaneous T cell lymphoma. Nat. Rev. Dis. Primers 7(1), 61 (2021). - PubMed
-
•• Provides a comprehensive and sophisticated discussion of cutaneous T-cell lymphoma (CTCL), spanning from mechanistic understanding of the disease to clinical presentation and treatment.
-
- Willemze R, Hodak E, Zinzani PL, Specht L, Ladetto M. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 29, iv30–iv40 (2018). - PubMed
-
- Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT. Long-term outcome of 525 patients with mycosis fungoides and Sézary syndrome: clinical prognostic factors and risk for disease progression. Arch. Dermatol. 139(7), 857–866 (2003). - PubMed
-
- Agar NS, Wedgeworth E, Crichton S et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary Syndrome: validation of the Revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer Staging Proposal. J. Clin. Oncol. 28(31), 4730–4739 (2010). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical