

Landiolol and Organ Failure in Patients With Septic Shock: The STRESS-L Randomized Clinical Trial
- PMID: 37877587
- PMCID: PMC10600724
- DOI: 10.1001/jama.2023.20134
Landiolol and Organ Failure in Patients With Septic Shock: The STRESS-L Randomized Clinical Trial
Abstract
Importance: Patients with septic shock undergo adrenergic stress, which affects cardiac, immune, inflammatory, and metabolic pathways. β-Blockade may attenuate the adverse effects of catecholamine exposure and has been associated with reduced mortality.
Objectives: To assess the efficacy and safety of landiolol in patients with tachycardia and established septic shock requiring prolonged (>24 hours) vasopressor support.
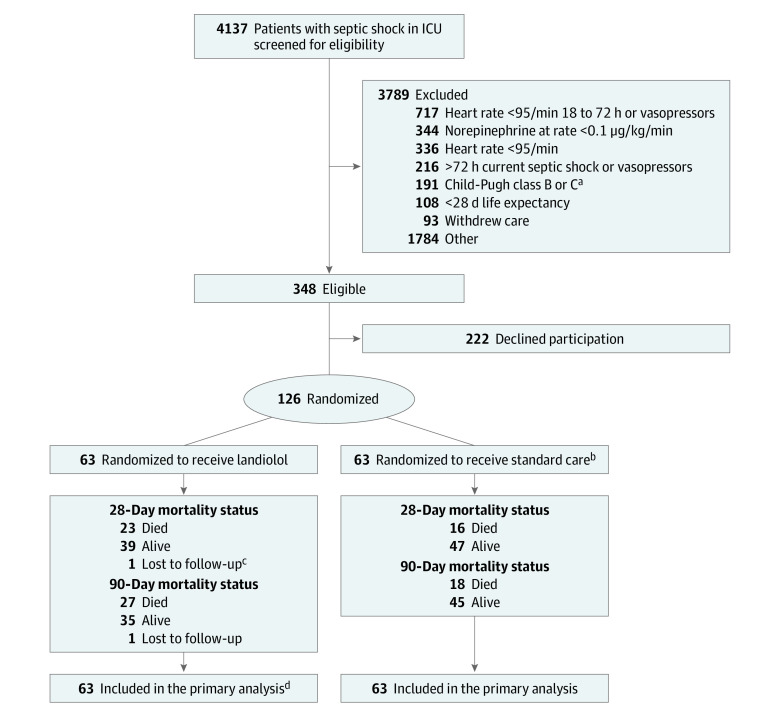
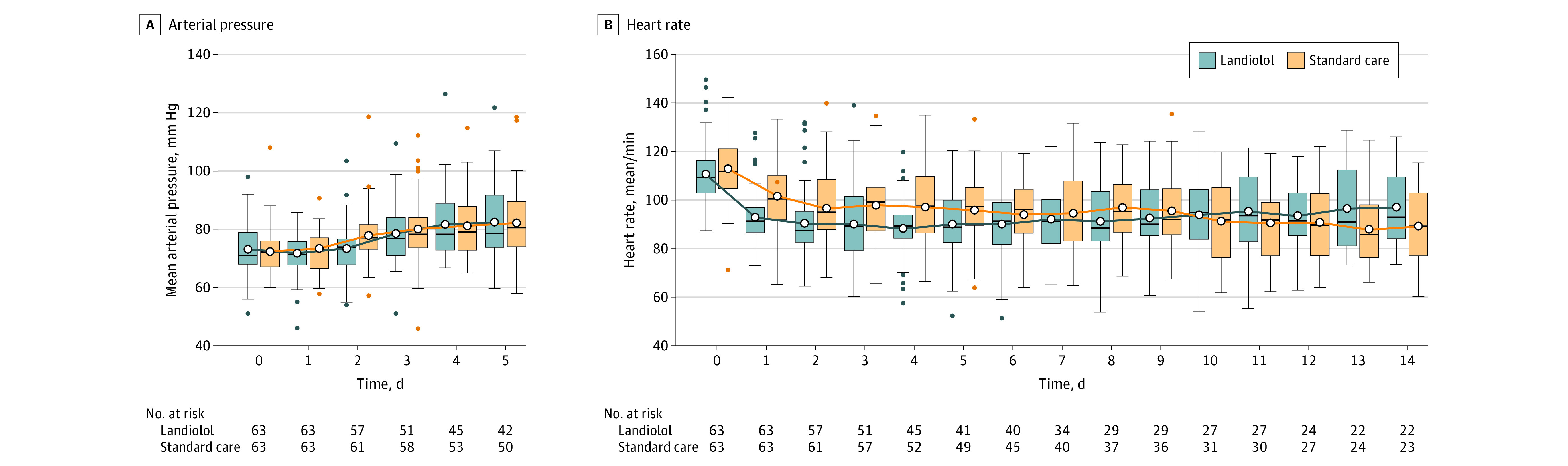
Design, setting, and participants: An open-label, multicenter, randomized trial involving 126 adults (≥18 years) with tachycardia (heart rate ≥95/min) and established septic shock treated for at least 24 hours with continuous norepinephrine (≥0.1 μg/kg/min) in 40 UK National Health Service intensive care units. The trial ran from April 2018 to December 2021, with early termination in December 2021 due to a signal of possible harm.
Intervention: Sixty-three patients were randomized to receive standard care and 63 to receive landiolol infusion.
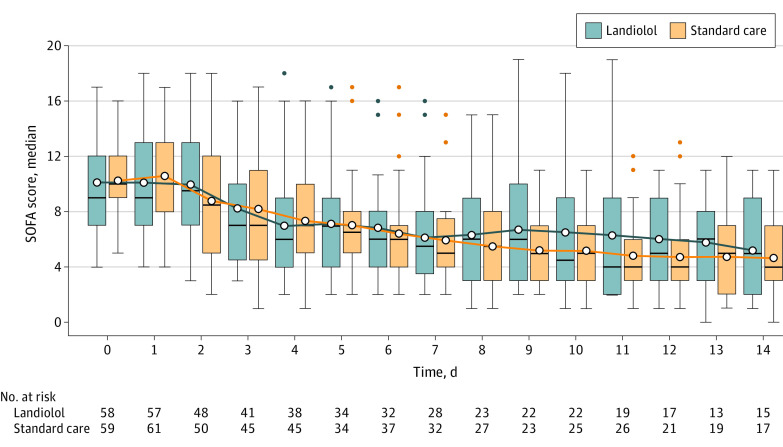
Main outcomes and measures: The primary outcome was the mean Sequential Organ Failure Assessment (SOFA) score from randomization through 14 days. Secondary outcomes included mortality at days 28 and 90 and the number of adverse events in each group.
Results: The trial was stopped prematurely on the advice of the independent data monitoring committee because it was unlikely to demonstrate benefit and because of possible harm. Of a planned 340 participants, 126 (37%) were enrolled (mean age, 55.6 years [95% CI, 52.7 to 58.5 years]; 58.7% male). The mean (SD) SOFA score in the landiolol group was 8.8 (3.9) compared with 8.1 (3.2) in the standard care group (mean difference [MD], 0.75 [95% CI, -0.49 to 2.0]; P = .24). Mortality at day 28 after randomization in the landiolol group was 37.1% (23 of 62) and 25.4% (16 of 63) in the standard care group (absolute difference, 11.7% [95% CI, -4.4% to 27.8%]; P = .16). Mortality at day 90 after randomization was 43.5% (27 of 62) in the landiolol group and 28.6% (18 of 63) in the standard care group (absolute difference, 15% [95% CI, -1.7% to 31.6%]; P = .08). There were no differences in the number of patients having at least one adverse event.
Conclusion and relevance: Among patients with septic shock with tachycardia and treated with norepinephrine for more than 24 hours, an infusion of landiolol did not reduce organ failure measured by the SOFA score over 14 days from randomization. These results do not support the use of landiolol for managing tachycardia among patients treated with norepinephrine for established septic shock.
Trial registration: EU Clinical Trials Register Eudra CT: 2017-001785-14; isrctn.org Identifier: ISRCTN12600919.
Conflict of interest statement
Figures
Comment in
-
β-Blockers in Patients With Sepsis: Putting the Puzzle Together, Piece by Piece.JAMA. 2023 Nov 7;330(17):1627-1628. doi: 10.1001/jama.2023.20455. JAMA. 2023. PMID: 37877588 No abstract available.
-
Use of Landiolol for Patients With Septic Shock and Organ Failure.JAMA. 2024 Feb 27;331(8):705. doi: 10.1001/jama.2023.27647. JAMA. 2024. PMID: 38411653 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
