

Comprehensive validation of early diagnostic algorithms for myocardial infarction in the emergency department
- PMID: 37878823
- PMCID: PMC10972704
- DOI: 10.1093/qjmed/hcad242
Comprehensive validation of early diagnostic algorithms for myocardial infarction in the emergency department
Abstract
Objective: To comprehensively evaluate diagnostic algorithms for myocardial infarction using a high-sensitivity cardiac troponin I (hs-cTnI) assay.
Patients and methods: We prospectively enrolled patients with suspected myocardial infarction without ST-segment elevation from nine emergency departments in Japan. The diagnostic algorithms evaluated: (i) based on hs-cTnI alone, such as the European Society of Cardiology (ESC) 0/1-h or 0/2-h and High-STEACS pathways; or (ii) used medical history and physical findings, such as the ADAPT, EDACS, HEART, and GRACE pathways. We evaluated the negative predictive value (NPV), sensitivity as safety measures, and proportion of patients classified as low or high-risk as an efficiency measure for a primary outcome of type 1 myocardial infarction or cardiac death within 30 days.
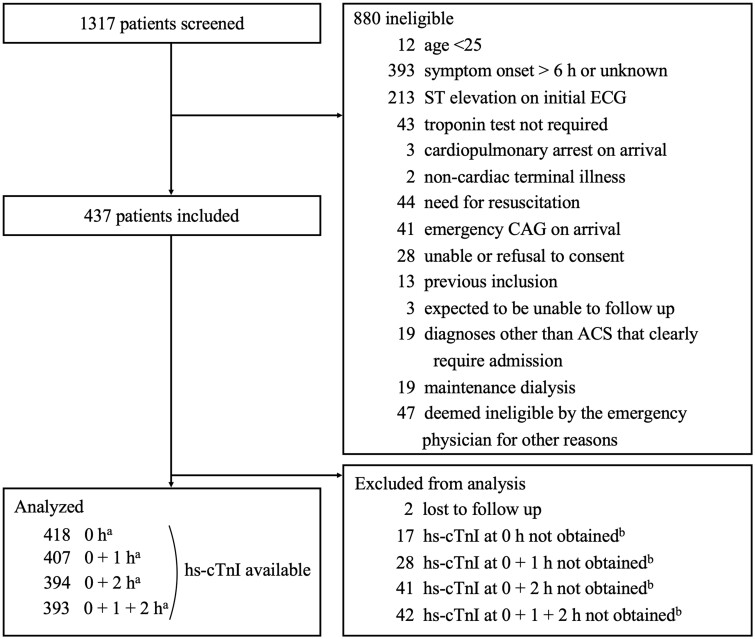
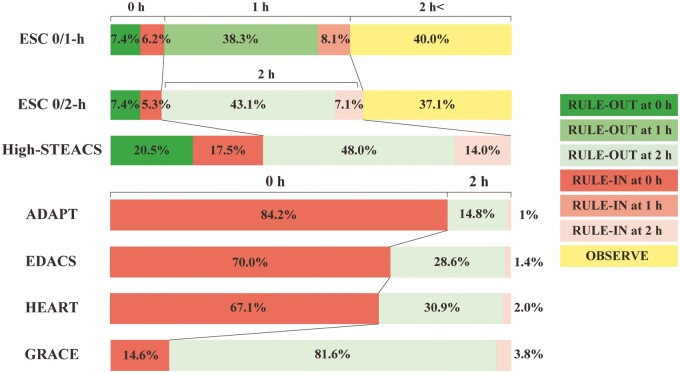
Results: We included 437 patients, and the hs-cTnI was collected at 0 and 1 hours in 407 patients and at 0 and 2 hours in 394. The primary outcome occurred in 8.1% (33/407) and 6.9% (27/394) of patients, respectively. All the algorithms classified low-risk patients without missing those with the primary outcome, except for the GRACE pathway. The hs-cTnI-based algorithms classified more patients as low-risk: the ESC 0/1-h 45.7%; the ESC 0/2-h 50.5%; the High-STEACS pathway 68.5%, than those using history and physical findings (15-30%). The High-STEACS pathway ruled out more patients (20.5%) by hs-cTnI measurement at 0 hours than the ESC 0/1-h and 0/2-h algorithms (7.4%).
Conclusions: The hs-cTnI algorithms, especially the High-STEACS pathway, had excellent safety performance for the early diagnosis of myocardial infarction and offered the greatest improvement in efficiency.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Association of Physicians.
Conflict of interest statement
M.T. received non-financial support from Abbott Japan, Roche Diagnostics, and Siemens Healthineers during the conduct of the study. These organizations did not contribute to the study design, the data analysis, the manuscript preparation, or publication decision. H.T. has received research grants or honoraria from Daiichi Sankyo, Biotronik Japan, Bristol Myers Squibb, Boehringer Ingelheim Japan, Novartis Japan, Medtronic Japan, Abbott Medical Japan, Medius Holdings, but all outside the study. N.L.M. has received research grants, honoraria or consultancy from Abbott Diagnostics, Roche Diagnostics, Siemens Healthineers, and LumiraDx, but none that supported this research. T.A.F. reports personal fees from DT Axis, Kyoto University Original, MSD and SONY, and a grant from Shionogi, outside the submitted work; In addition, T.A.F. has patents 2020-548587 and 2022-082495 pending, and intellectual properties for Kokoro-app licensed to Mitsubishi-Tanabe. The remaining authors have nothing to disclose.
Figures
Similar articles
-
Accelerated diagnostic pathways for myocardial infarction using a Siemens High-Sensitivity cardiac troponin I assay.Clin Biochem. 2025 Mar;136:110897. doi: 10.1016/j.clinbiochem.2025.110897. Epub 2025 Feb 14. Clin Biochem. 2025. PMID: 39956308
-
Diagnostic accuracy of a machine learning algorithm using point-of-care high-sensitivity cardiac troponin I for rapid rule-out of myocardial infarction: a retrospective study.Lancet Digit Health. 2024 Oct;6(10):e729-e738. doi: 10.1016/S2589-7500(24)00191-2. Epub 2024 Aug 29. Lancet Digit Health. 2024. PMID: 39214763
-
Combining High-Sensitivity Cardiac Troponin I and Cardiac Troponin T in the Early Diagnosis of Acute Myocardial Infarction.Circulation. 2018 Sep 4;138(10):989-999. doi: 10.1161/CIRCULATIONAHA.117.032003. Circulation. 2018. PMID: 29691270
-
High-sensitivity-cardiac troponin for accelerated diagnosis of acute myocardial infarction: A systematic review and meta-analysis.Am J Emerg Med. 2020 Jul;38(7):1402-1407. doi: 10.1016/j.ajem.2019.11.035. Epub 2019 Dec 28. Am J Emerg Med. 2020. PMID: 31932131
-
Safety and efficacy of the European Society of Cardiology 0/1-hour algorithm for diagnosis of myocardial infarction: systematic review and meta-analysis.Heart. 2020 Jul;106(13):985-991. doi: 10.1136/heartjnl-2019-316343. Epub 2020 Apr 3. Heart. 2020. PMID: 32245882
References
-
- Levy PD, Mahler SA.. Evaluating suspected acute MI in the emergency department: what is and what should never be. J Am Coll Cardiol 2019; 74:495–7. - PubMed
-
- Twerenbold R, Neumann JT, Sorensen NA, Ojeda F, Karakas M, Boeddinghaus J, et al.Prospective validation of the 0/1-h algorithm for early diagnosis of myocardial infarction. J Am Coll Cardiol 2018; 72:620–32. - PubMed
-
- Collet JP, Thiele H, Barbato E, Barthelemy O, Bauersachs J, Bhatt DL, et al.; ESC Scientific Document Group. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2021; 42:1289–367. - PubMed
-
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al.2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021; 144:e368–e54. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
