

A Systematic Review of Predictor Composition, Outcomes, Risk of Bias, and Validation of COVID-19 Prognostic Scores
- PMID: 37879096
- PMCID: PMC11006104
- DOI: 10.1093/cid/ciad618
A Systematic Review of Predictor Composition, Outcomes, Risk of Bias, and Validation of COVID-19 Prognostic Scores
Abstract
Background: Numerous prognostic scores have been published to support risk stratification for patients with coronavirus disease 2019 (COVID-19).
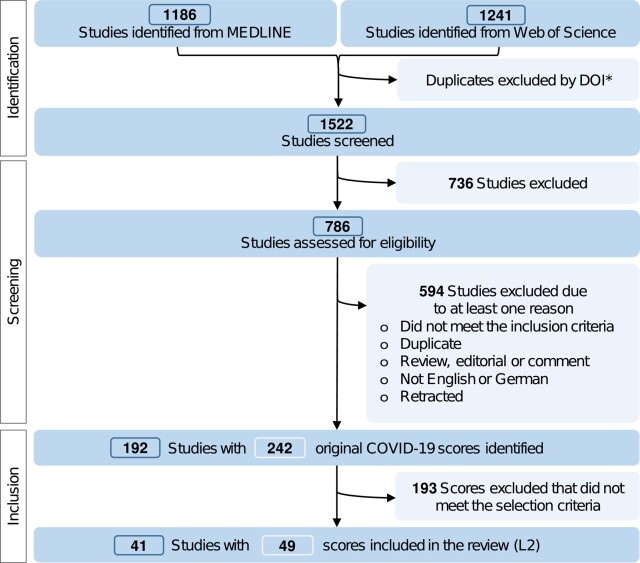
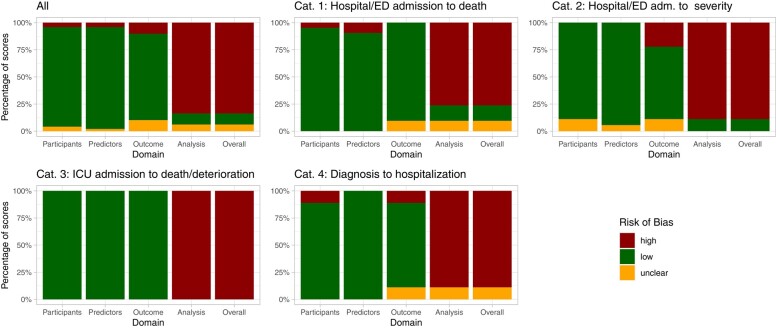
Methods: We performed a systematic review to identify the scores for confirmed or clinically assumed COVID-19 cases. An in-depth assessment and risk of bias (ROB) analysis (Prediction model Risk Of Bias ASsessment Tool [PROBAST]) was conducted for scores fulfilling predefined criteria ([I] area under the curve [AUC)] ≥ 0.75; [II] a separate validation cohort present; [III] training data from a multicenter setting [≥2 centers]; [IV] point-scale scoring system).
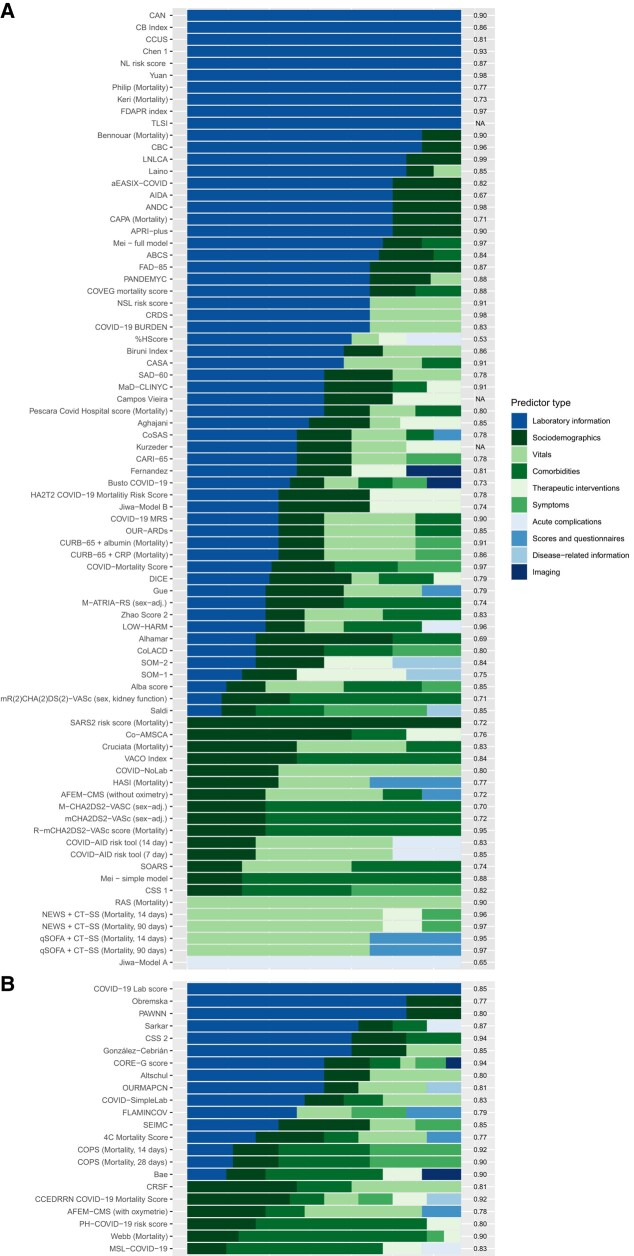
Results: Out of 1522 studies extracted from MEDLINE/Web of Science (20/02/2023), we identified 242 scores for COVID-19 outcome prognosis (mortality 109, severity 116, hospitalization 14, long-term sequelae 3). Most scores were developed using retrospective (75.2%) or single-center (57.1%) cohorts. Predictor analysis revealed the primary use of laboratory data and sociodemographic information in mortality and severity scores. Forty-nine scores were included in the in-depth analysis. The results indicated heterogeneous quality and predictor selection, with only five scores featuring low ROB. Among those, based on the number and heterogeneity of validation studies, only the 4C Mortality Score can be recommended for clinical application so far.
Conclusions: The application and translation of most existing COVID scores appear unreliable. Guided development and predictor selection would have improved the generalizability of the scores and may enhance pandemic preparedness in the future.
Keywords: COVID-19; pandemic preparedness; prediction models; predictors; scores.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. J. J. V. received research funding and consulting fees from Merck/MSD, Gilead, Pfizer, Astellas Pharma, Basilea, German Centre for Infection Research (DZIF), University Hospital Freiburg/Congress and Communication, Academy for Infectious Medicine, University Manchester, German Society for Infectious Diseases (DGI), German Federal Ministry of Education and Research (BMBF), Deutsches Zentrum für Luft- und Raumfahrt (DLR), University of Bristol, Rigshospitalet Copenhagen; consulting fees from Ärztekammer Nordrhein, University Hospital Aachen, Back Bay Strategies, German Society for Internal Medicine (DGIM), Shionogi, Molecular Health, Netzwerk Universitätsmedizin, Janssen, NordForsk, Biontech, APOGEPHA; and reports participation on Data Safety Monitoring or Advisory Boards for APOGEPHA Arzneimittel, Biontech, Merck/MSD, Gilead, and Pfizer. D. M. received speaker honoraria from Free University of Berlin and travel compensation from IQVIA. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- Therapeutics and COVID-19: living guideline, 13 January 2023. Geneva: World Health Organization, 2023. (WHO/2019-nCoV/therapeutics/2023.1). Licence: CC BY-NC-SA 3.0 IGO. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
