Metabolomic profiling of preterm birth in pregnant women living with HIV
- PMID: 37880481
- PMCID: PMC10600291
- DOI: 10.1007/s11306-023-02055-1
Metabolomic profiling of preterm birth in pregnant women living with HIV
Abstract
Background: Preterm birth is a leading cause of death in children under the age of five. The risk of preterm birth is increased by maternal HIV infection as well as by certain antiretroviral regimens, leading to a disproportionate burden on low- and medium-income settings where HIV is most prevalent. Despite decades of research, the mechanisms underlying spontaneous preterm birth, particularly in resource limited areas with high HIV infection rates, are still poorly understood and accurate prediction and therapeutic intervention remain elusive.
Objectives: Metabolomics was utilized to identify profiles of preterm birth among pregnant women living with HIV on two different antiretroviral therapy (ART) regimens.
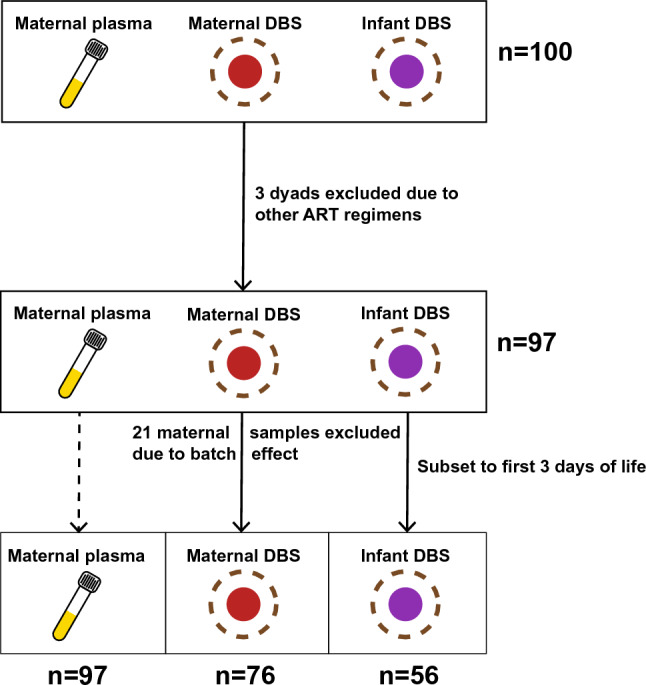
Methods: This pilot study comprised 100 mother-infant dyads prior to antiretroviral initiation, on zidovudine monotherapy or on protease inhibitor-based antiretroviral therapy. Pregnancies that resulted in preterm births were matched 1:1 with controls by gestational age at time of sample collection. Maternal plasma and blood spots at 23-35 weeks gestation and infant dried blood spots at birth, were assayed using an untargeted metabolomics method. Linear regression and random forests classification models were used to identify shared and treatment-specific markers of preterm birth.
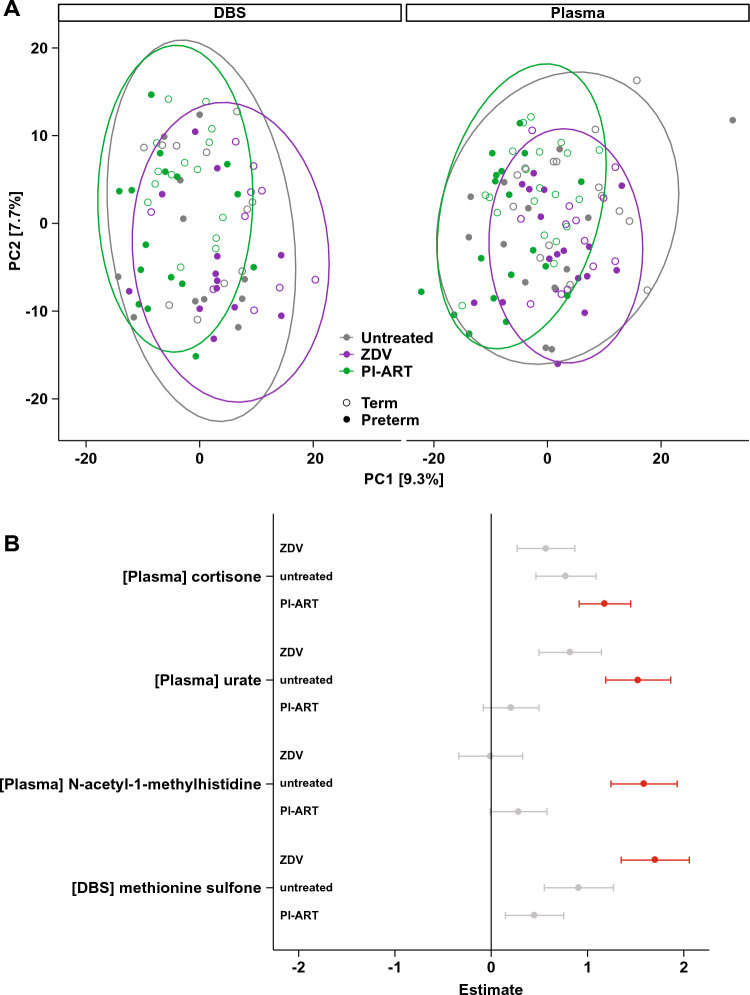
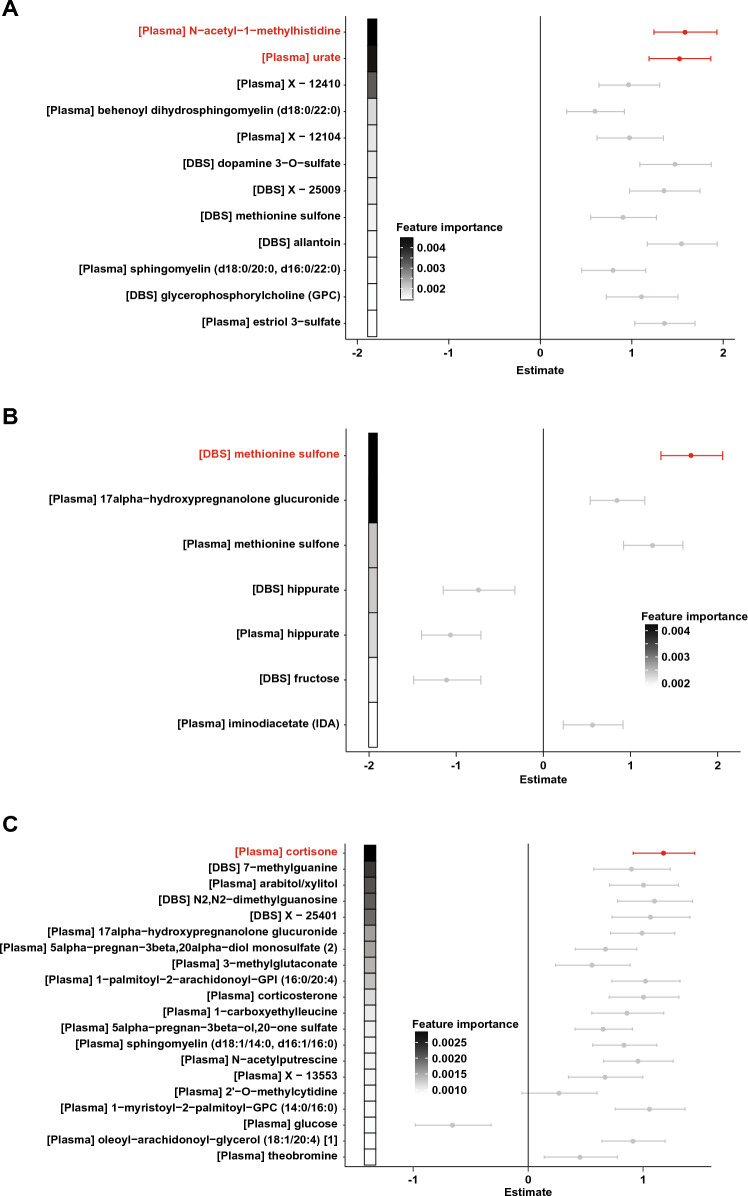
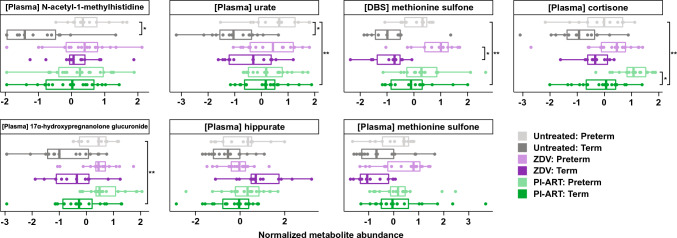
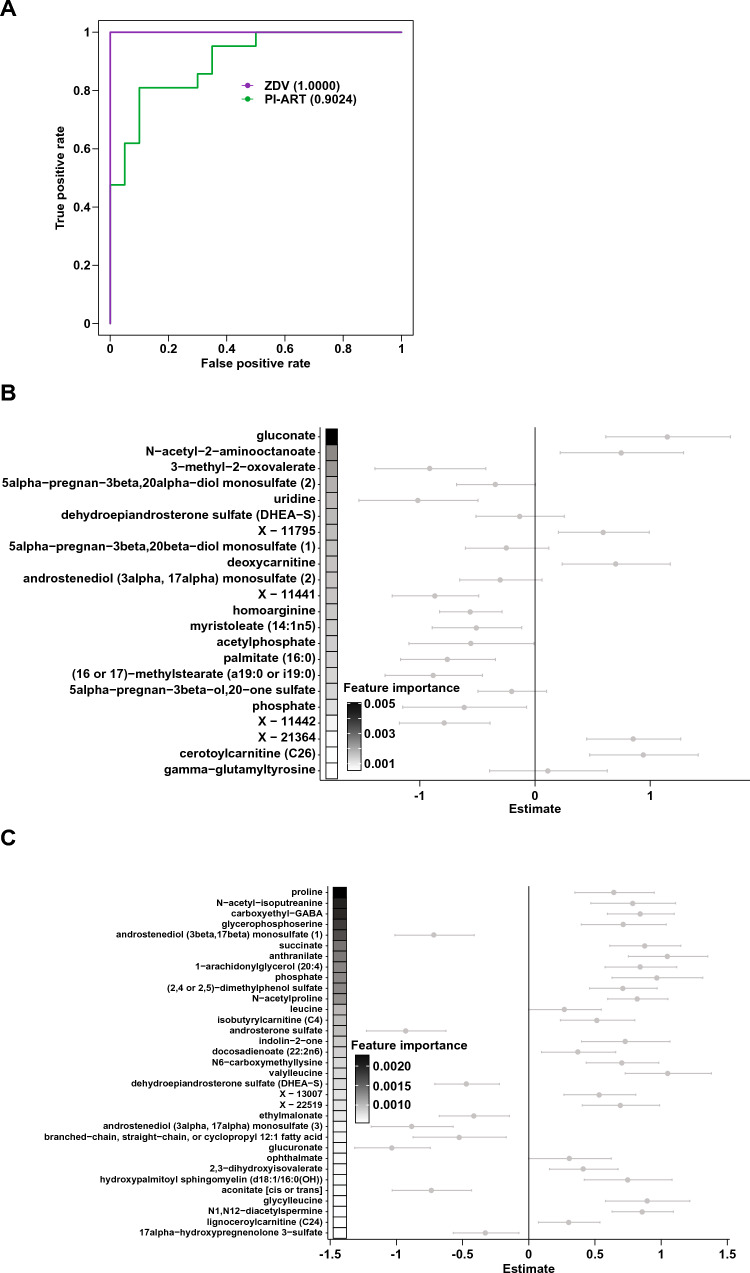
Results: Classification models for preterm birth achieved accuracies of 95.5%, 95.7%, and 80.7% in the untreated, zidovudine monotherapy, and protease inhibitor-based treatment groups, respectively. Urate, methionine sulfone, cortisone, and 17α-hydroxypregnanolone glucuronide were identified as shared markers of preterm birth. Other compounds including hippurate and N-acetyl-1-methylhistidine were found to be significantly altered in a treatment-specific context.
Conclusion: This study identified previously known as well as novel metabolomic features of preterm birth in pregnant women living with HIV. Validation of these models in a larger, independent cohort is necessary to ascertain whether they can be utilized to predict preterm birth during a stage of gestation that allows for therapeutic intervention or more effective resource allocation.
Keywords: Dried blood spots; Metabolomics; Plasma; Preterm birth; Women living with HIV; Zidovudine.
© 2023. The Author(s).
Conflict of interest statement
The authors report no conflict of interest.
Figures