

UK Kidney Association Clinical Practice Guideline: Sodium-Glucose Co-transporter-2 (SGLT-2) Inhibition in Adults with Kidney Disease 2023 UPDATE
- PMID: 37880609
- PMCID: PMC10598949
- DOI: 10.1186/s12882-023-03339-3
UK Kidney Association Clinical Practice Guideline: Sodium-Glucose Co-transporter-2 (SGLT-2) Inhibition in Adults with Kidney Disease 2023 UPDATE
Abstract
Large placebo-controlled trials have demonstrated kidney and cardiovascular clinical benefits of SGLT-2 inhibitors. Data from the EMPA-KIDNEY and DELIVER trials and associated meta-analyses triggered an update to the UK Kidney Association Clinical Practice Guideline on Sodium-Glucose Co-transporter-2 (SGLT-2) Inhibition in Adults with Kidney Disease. We provide a summary of the full guideline and highlight the rationale for recent updates. The use of SGLT-2 inhibitors in people with specific medical conditions, including type 1 diabetes, kidney transplants, and people admitted to hospital with heart failure is also considered, along with Recommendations for future research and Recommendations for implementation. A full "lay" summary of the guidelines is provided as an appendix to ensure that these guidelines are accessible and understandable to people who are not medical professionals.
Keywords: Acute kidney injury; Chronic kidney disease; Gliflozin; Guideline.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
SB reports honoraria for lectures, presentations and speaker bureaus from Astra Zeneca. JOB reports a leadership position as chair of the UK Kidney Association Clinical Practice Guidelines Committee and reports honoraria for speaker bureaus from AstraZeneca, Boehringer-Ingelheim and NAPP. CC reports support from North East London Integrated Care Board, Clinical Effectiveness Group, Queen Mary University of London, and National Institute of Health Research, and reports a grant or contract from the NIHR School of Primary Care Research. MEK reports participation on advisory boards for GlaxoSmithKline and Astella. AHF reports an institutional grant from Boehringer-Ingelheim for participation in the EMPA-KIDNEY study, honoraria or personal fees from Boehringer-Ingelheim and AstraZeneca, support for attending meetings from AstraZeneca, and participation in advisory boards for Boehringer-Ingelheim and AstraZeneca. DF reports unpaid leadership roles with the American Society of Nephrology Education Committee, EuroPD management board, and the International Society of Peritoneal Dialysis Programme Committee. MH reports honoraria from AstraZeneca and UK Renal Pharmacy Group. PH reports a personal grant from Roche Diagnostics, honoraria or personal fees from AstraZeneca, NovoNordisk and Boehringer-Ingelheim, and participation in data safety monitoring board or advisory boards for Abbott, AstraZeneca, and Bayer. AJR, WGH and NS report institutional grant funding from Boehringer-Ingelheim and Eli Lilly. NS additionally reports institutional grant funding from NovoNordisk. WGH additionally reports funding from the UK Medical Research Council–Kidney Research UK Professor David Kerr Clinician Scientist Award. AWa reports honoraria and support for travel expenses from GlaxoSmithKline. DW reports honoraria from ABCD and Sanofi Aventis and reports participation in a data safety monitoring board or advisory board for the BARI 2 study. AWo reports honoraria from Bayer and AstraZeneca and participant in advisory board for Bayer. AK, EL, MAW, and AR have no competing interests to declare.
Figures
References
-
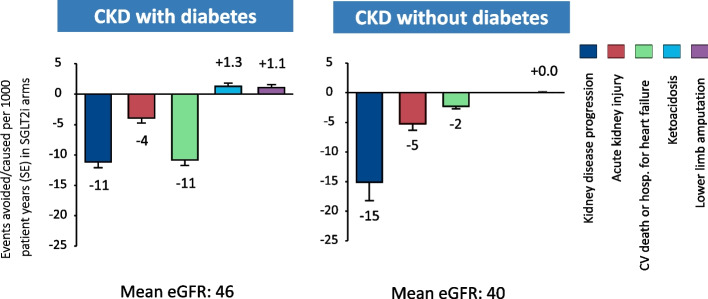
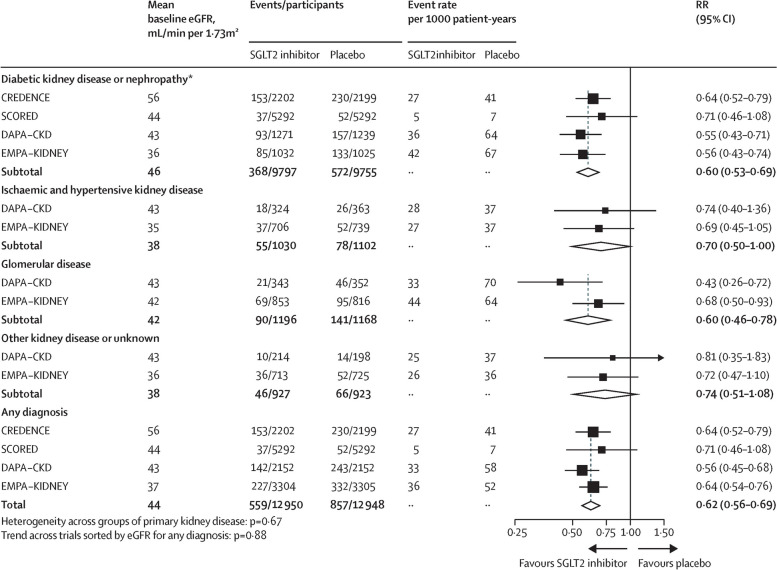
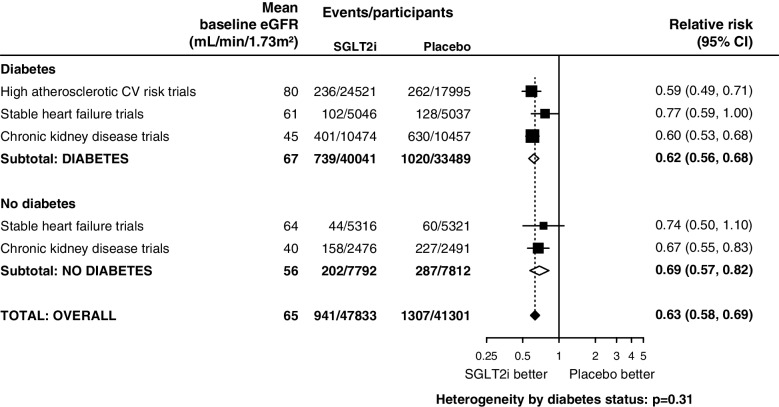
- Nuffield Department of Population Health Renal Studies Group and the SGLT2 inhibitor Meta-Analysis Cardio-Renal Trialists' Consortium Impact of diabetes on the effects of sodium glucose co-transporter-2 inhibitors on kidney outcomes: collaborative meta-analysis of large placebo-controlled trials. Lancet. 2022;400(10365):1788–801. doi: 10.1016/S0140-6736(22)02074-8. - DOI - PMC - PubMed
-
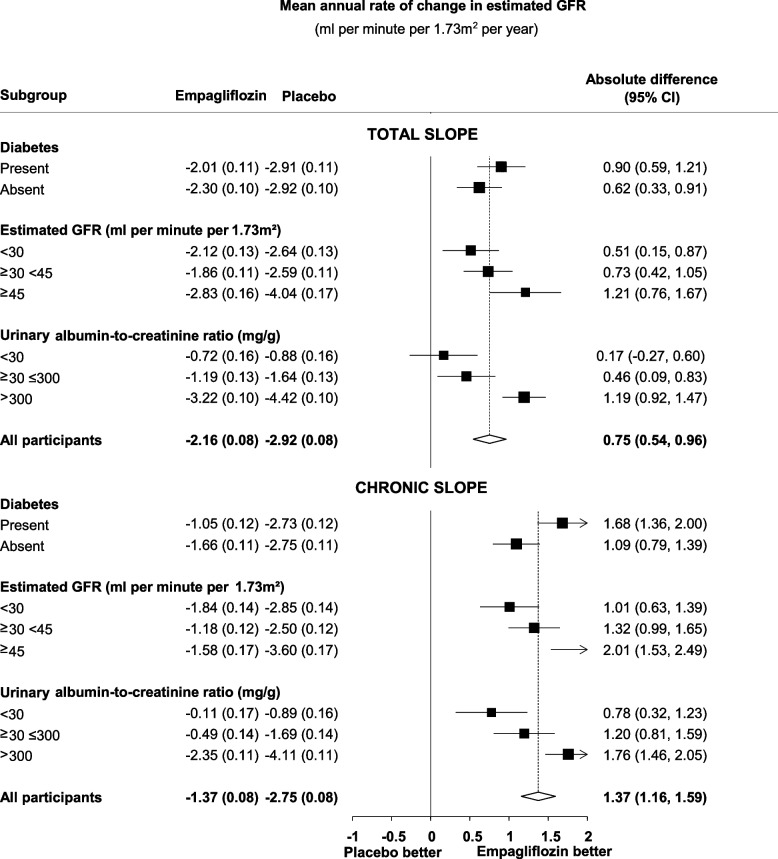
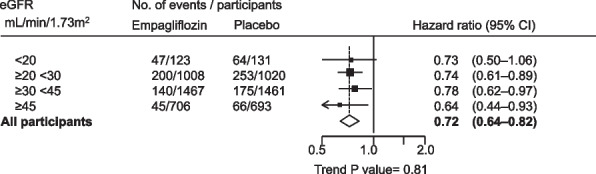
- Staplin N, Roddick AJ, Emberson J, Reith C, Riding A, Wonnacott A, et al. Net effects of sodium-glucose co-transporter-2 inhibition in different patient groups: a meta-analysis of large placebo-controlled randomized trials. EClinicalMedicine. 2021;41:101163. doi: 10.1016/j.eclinm.2021.101163. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
