

Mechanical thrombectomy in intermediate- and high-risk acute pulmonary embolism: hemodynamic outcomes at three months
- PMID: 37880651
- PMCID: PMC10601326
- DOI: 10.1186/s12931-023-02552-w
Mechanical thrombectomy in intermediate- and high-risk acute pulmonary embolism: hemodynamic outcomes at three months
Abstract
Background: Mechanical thrombectomy has been shown to reduce thrombus burden and pulmonary artery pressure (PAP) and to improve right ventricular (RV) function in patients with high-risk or intermediate-high-risk pulmonary embolism (PE). As hemodynamic data after mechanical thrombectomy for PE are scarce, we aimed to assess the hemodynamic effects of mechanical thrombectomy in acute PE with right heart overload.
Methods: In this prospective, open-label study, patients with acute symptomatic, computed tomography-documented PE with signs of right heart overload underwent mechanical thrombectomy using the FlowTriever System. Right heart catheterization was performed immediately before and after thrombectomy and after three months. Transthoracic echocardiography was performed before thrombectomy, discharge, and at three months. This analysis was done after 20 patients completed three months of follow-up.
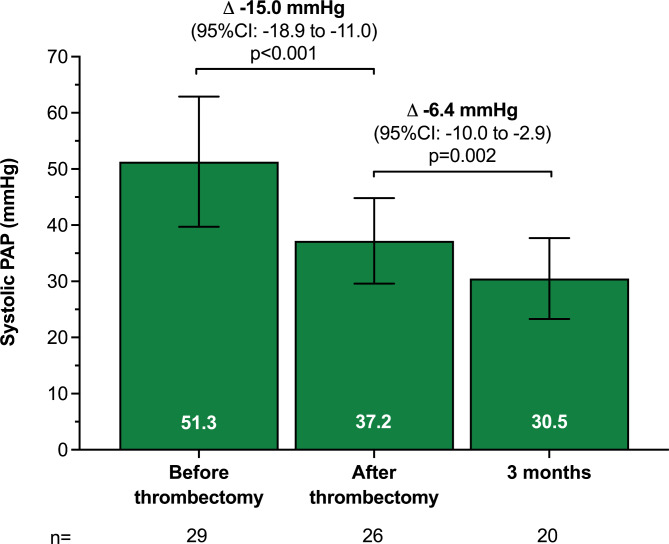
Results: Twenty-nine patients (34% female) underwent mechanical thrombectomy, of which 20 completed three months follow-up with right heart catheterization. Most patients were at high (17%) or intermediate-high (76%) risk and had bilateral PE (79%). Before thrombectomy, systolic PAP (sPAP) was severely elevated (mean 51.3 ± 11.6 mmHg). Mean sPAP dropped by -15.0 mmHg (95% confidence interval [CI]: -18.9 to -11.0; p < 0.001) immediately after the procedure and continued to decrease from post-thrombectomy to three months (-6.4 mmHg, 95% CI: -10-0 to -2.9; p = 0.002). RV/left ventricular (LV) ratio immediately reduced within two days by -0.37 (95% CI: -0.47 to -0.27; p < 0.001). The proportion of patients with a tricuspid annular plane systolic excursion (TAPSE)/sPAP ratio < 0.31 mm/mmHg decreased from 28% at baseline to 0% before discharge and at three months (p = 0.007). There were no procedure-related major adverse events.
Conclusions: Mechanical thrombectomy for acute PE was safe and immediately reduced PAP and improved right heart function. The reduction in PAP was maintained at three months follow-up.
Keywords: Mechanical thrombectomy; Pulmonary embolism.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
LL received speaker honoraria from AstraZeneca, ReCor Medical and Medtronic. FG is supported by the German Foundation of Heart Research and has received speaker honoraria from Astra-Zeneca. SE received speaker honoraria and/or travel support from Akcea Therapeutics, AstraZeneca, Bayer, Berlin Chemie, Bristol-Myers Squibb, Pfizer, Böhringer Ingelheim, Daiichi Sankyo, Edwards Lifesciences, Inari medical, Kaneka Pharma, Medtronic, Novartis and Recor. MB is supported by the Deutsche Forschungsgemeinschaft (German Research Foundation; TTR 219, project number 322900939) and reports personal fees from Abbott, Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Edwards, Medtronic, Novartis, Recor, Servier and Vifor during the conduct of the study. FM is supported by Deutsche Gesellschaft für Kardiologie (DGK), Deutsche Forschungsgemeinschaft (SFB TRR219), and Deutsche Herzstiftung. He has received scientific support from Ablative Solutions, Medtronic and ReCor Medical and speaker honoraria/consulting fees from Ablative Solutions, Amgen, Astra-Zeneca, Bayer, Boehringer Ingelheim, Inari, Medtronic, Merck, ReCor Medical, Servier, and Terumo. PPN, HAG, BH, PL, SK, AL, and BS report no conflict of interest related to this study.
Figures
References
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the european respiratory society (ERS) Eur Heart J. 2020;41(4):543–603. doi: 10.1093/eurheartj/ehz405. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
