

Cost-effectiveness analysis of surgical proximal femur fracture prevention in elderly: a Markov cohort simulation model
- PMID: 37880692
- PMCID: PMC10601292
- DOI: 10.1186/s12962-023-00482-4
Cost-effectiveness analysis of surgical proximal femur fracture prevention in elderly: a Markov cohort simulation model
Abstract
Background: Hip fractures are a common and costly health problem, resulting in significant morbidity and mortality, as well as high costs for healthcare systems, especially for the elderly. Implementing surgical preventive strategies has the potential to improve the quality of life and reduce the burden on healthcare resources, particularly in the long term. However, there are currently limited guidelines for standardizing hip fracture prophylaxis practices.
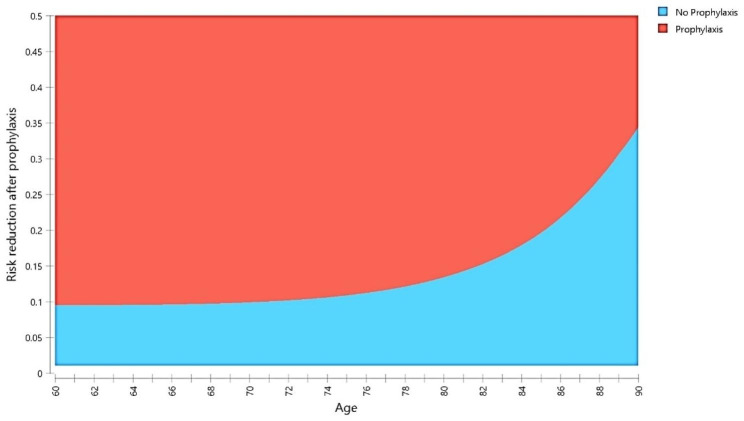
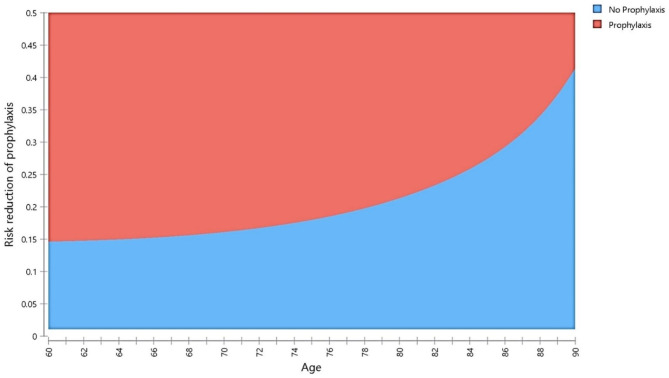
Methods: This study used a cost-effectiveness analysis with a finite-state Markov model and cohort simulation to evaluate the primary and secondary surgical prevention of hip fractures in the elderly. Patients aged 60 to 90 years were simulated in two different models (A and B) to assess prevention at different levels. Model A assumed prophylaxis was performed during the fracture operation on the contralateral side, while Model B included individuals with high fracture risk factors. Costs were obtained from the Centers for Medicare & Medicaid Services, and transition probabilities and health state utilities were derived from available literature. The baseline assumption was a 10% reduction in fracture risk after prophylaxis. A sensitivity analysis was also conducted to assess the reliability and variability of the results.
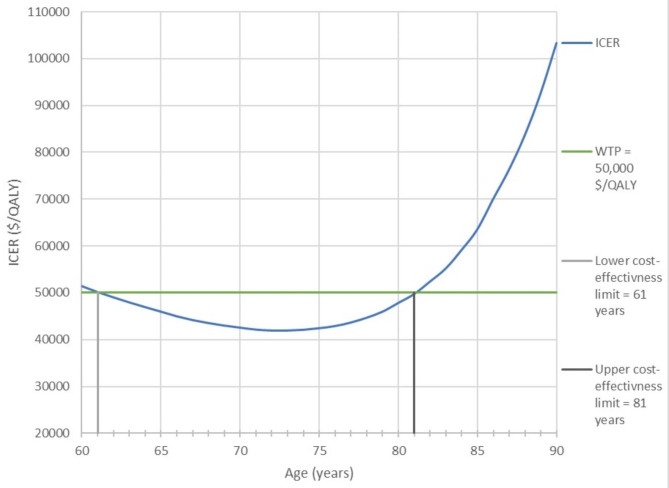
Results: With a 10% fracture risk reduction, model A costs between $8,850 and $46,940 per quality-adjusted life-year ($/QALY). Additionally, it proved most cost-effective in the age range between 61 and 81 years. The sensitivity analysis established that a reduction of ≥ 2.8% is needed for prophylaxis to be definitely cost-effective. The cost-effectiveness at the secondary prevention level was most sensitive to the cost of the contralateral side's prophylaxis, the patient's age, and fracture treatment cost. For high-risk patients with no fracture history, the cost-effectiveness of a preventive strategy depends on their risk profile. In the baseline analysis, the incremental cost-effectiveness ratio at the primary prevention level varied between $11,000/QALY and $74,000/QALY, which is below the defined willingness to pay threshold.
Conclusion: Due to the high cost of hip fracture treatment and its increased morbidity, surgical prophylaxis strategies have demonstrated that they can significantly relieve the healthcare system. Various key assumptions facilitated the modeling, allowing for adequate room for uncertainty. Further research is needed to evaluate health-state-associated risks.
Keywords: Cost-effectiveness; Finite-State Markov Model; Geriatric; Healthcare utilization; Hip fractures; Prevention; Prophylaxis; Quality-adjusted life-year; Sensitivity analysis; Surgical Prophylaxis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Department of Economic and Social Affairs. Population Division. World Population Ageing 2019. New York; 2020.
-
- United Nations. Ageing. 2020. https://www.un.org/en/sections/issues-depth/ageing/. Accessed 23 Oct 2020.
-
- Cummings SR, Rubin SM, Black D. The future of hip fractures in the United States. Numbers, costs, and potential effects of postmenopausal estrogen. CORR. 1990:163–6. - PubMed
LinkOut - more resources
Full Text Sources
