

Surgical management of craniospinal axis malignant peripheral nerve sheath tumors: a single-institution experience and literature review
- PMID: 37880773
- PMCID: PMC10601280
- DOI: 10.1186/s12957-023-03227-y
Surgical management of craniospinal axis malignant peripheral nerve sheath tumors: a single-institution experience and literature review
Abstract
Background: Malignant peripheral nerve sheath tumor (MPNST) is an exceedingly rare and aggressive tumor, with limited literature on its management. Herein, we present our series of surgically managed craniospinal MPNSTs, analyze their outcomes, and review the literature.
Methods: We retrospectively reviewed surgically managed primary craniospinal MPNSTs treated at our institution between January 2005 and May 2023. Patient demographics, tumor features, and treatment outcomes were assessed. Neurological function was quantified using the Frankel grade and Karnofsky performance scores. Descriptive statistics, rank-sum tests, and Kaplan-Meier survival analyses were performed.
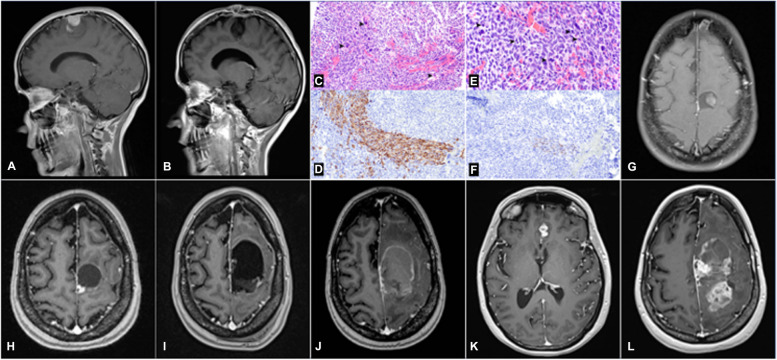
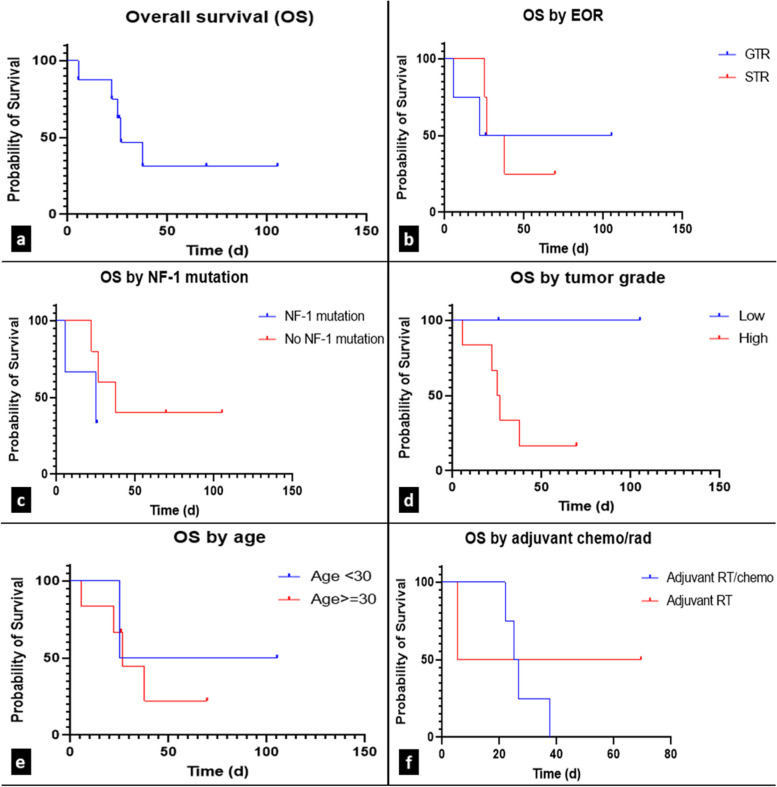
Results: Eight patients satisfied the inclusion criteria (4 male, 4 female). The median age at presentation was 38 years (range 15-67). Most tumors were localized to the spine (75%), and 3 patients had neurofibromatosis type 1. The most common presenting symptoms were paresthesia (50%) and visual changes (13%). The median tumor size was 3 cm, and most tumors were oval-shaped (50%) with well-defined borders (75%). Six tumors were high grade (75%), and gross total resection was achieved in 5 patients, with subtotal resection in the remaining 3 patients. Postoperative radiotherapy and chemotherapy were performed in 6 (75%) and 4 (50%) cases, respectively. Local recurrence occurred in 5 (63%) cases, and distant metastases occurred in 2 (25%). The median overall survival was 26.7 months. Five (63%) patients died due to recurrence.
Conclusions: Primary craniospinal MPNSTs are rare and have an aggressive clinical course. Early diagnosis and treatment are essential for managing these tumors. In this single-center study with a small cohort, maximal resection, low-grade pathology, young age (< 30), and adjuvant radiotherapy were associated with improved survival.
Keywords: Craniospinal axis; MPNST; Malignant Triton tumor; Malignant peripheral nerve sheath tumors; Mesenchymal tumors.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021;23:1231–1251. doi: 10.1093/neuonc/noab106. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
