

Implementing patient derived organoids in functional precision medicine for patients with advanced colorectal cancer
- PMID: 37880806
- PMCID: PMC10598932
- DOI: 10.1186/s13046-023-02853-4
Implementing patient derived organoids in functional precision medicine for patients with advanced colorectal cancer
Abstract
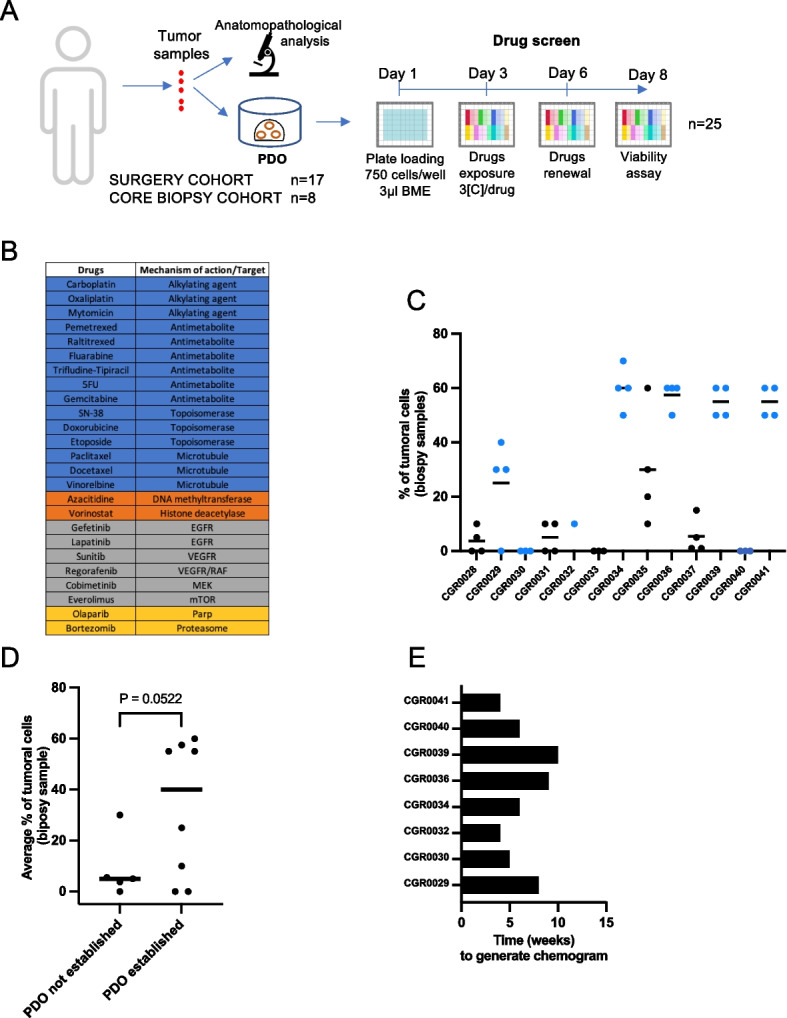
Background: Patient Derived Organoids (PDOs) emerged as the best technology to develop ex vivo tumor avatars. Whether drug testing on PDOs to identify efficient therapies will bring clinical utility by improving patient survival remains unclear. To test this hypothesis in the frame of clinical trials, PDO technology faces three main challenges to be implemented in routine clinical practices: i) generating PDOs with a limited amount of tumor material; ii) testing a wide panel of anti-cancer drugs; and iii) obtaining results within a time frame compatible with patient disease management. We aimed to address these challenges in a prospective study in patients with colorectal cancer (CRC).
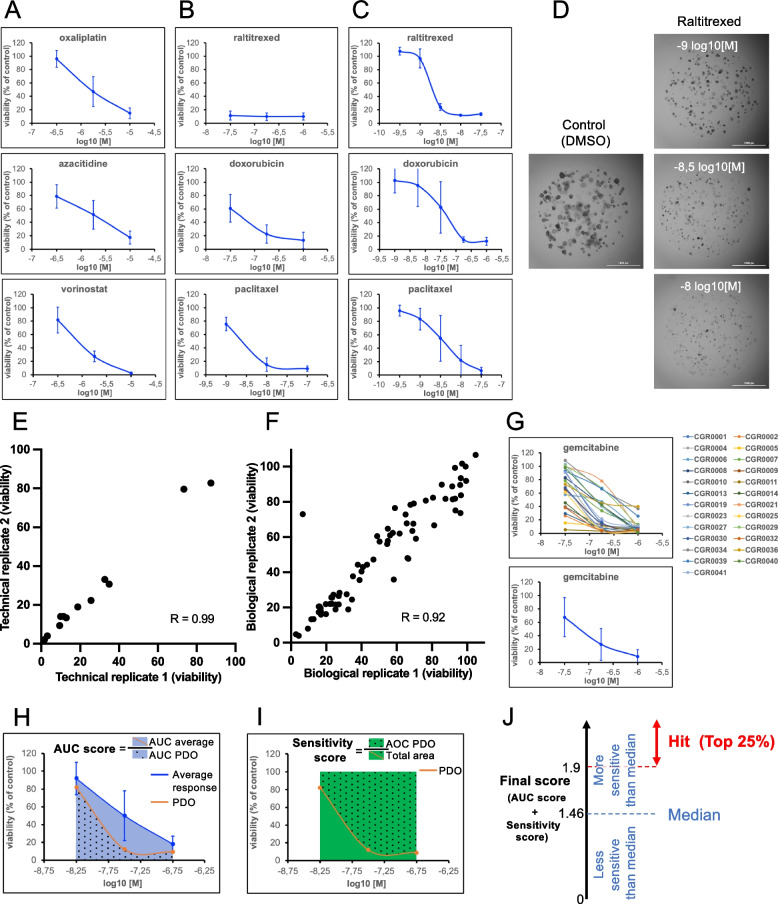
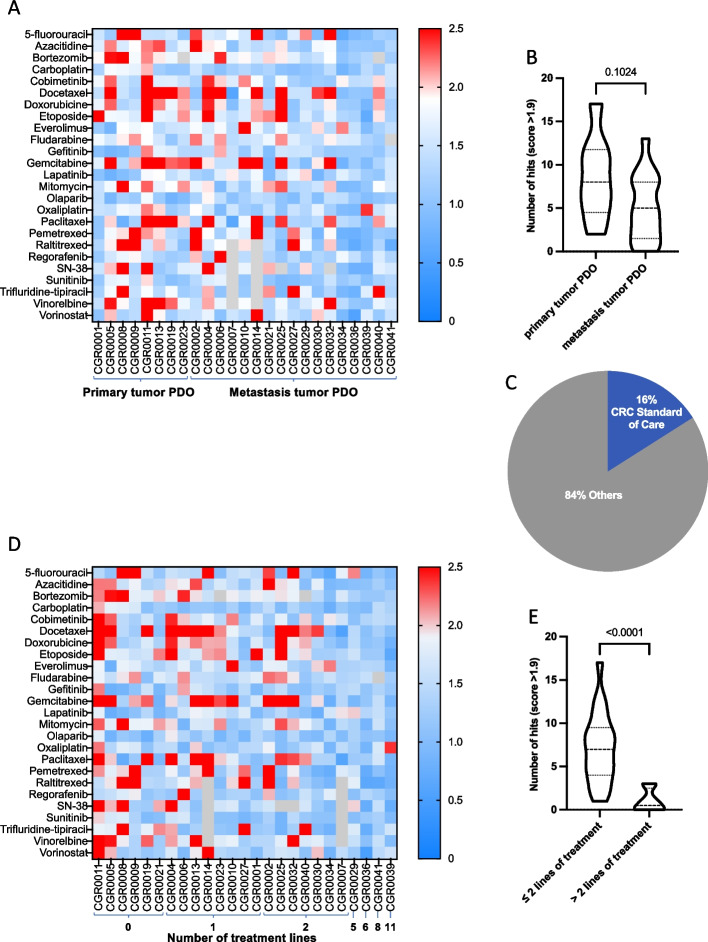
Methods: Fresh surgical or core needle biopsies were obtained from patients with CRC. PDOs were established and challenged with a panel of 25 FDA-approved anti-cancer drugs (chemotherapies and targeted therapies) to establish a scoring method ('chemogram') identifying in vitro responders. The results were analyzed at the scale of the cohort and individual patients when the follow-up data were available.
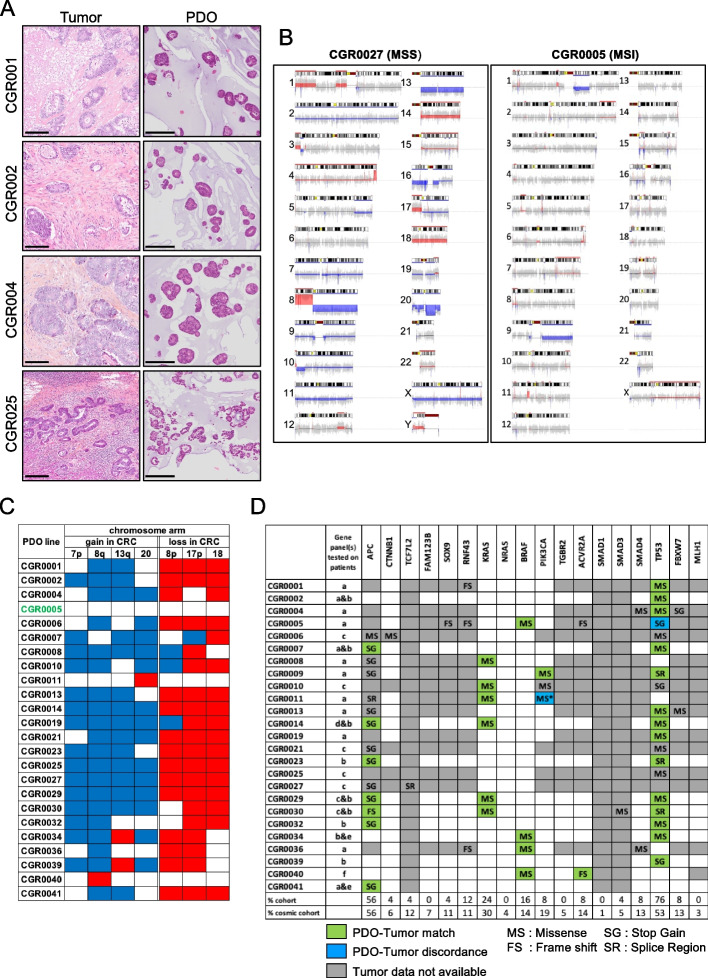
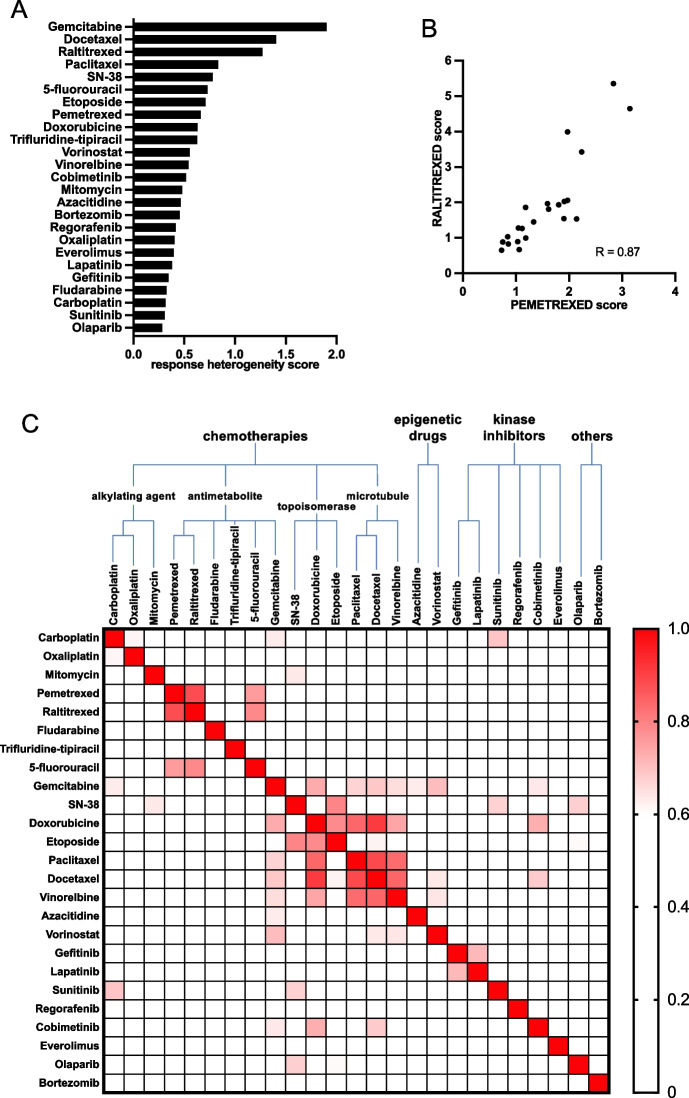
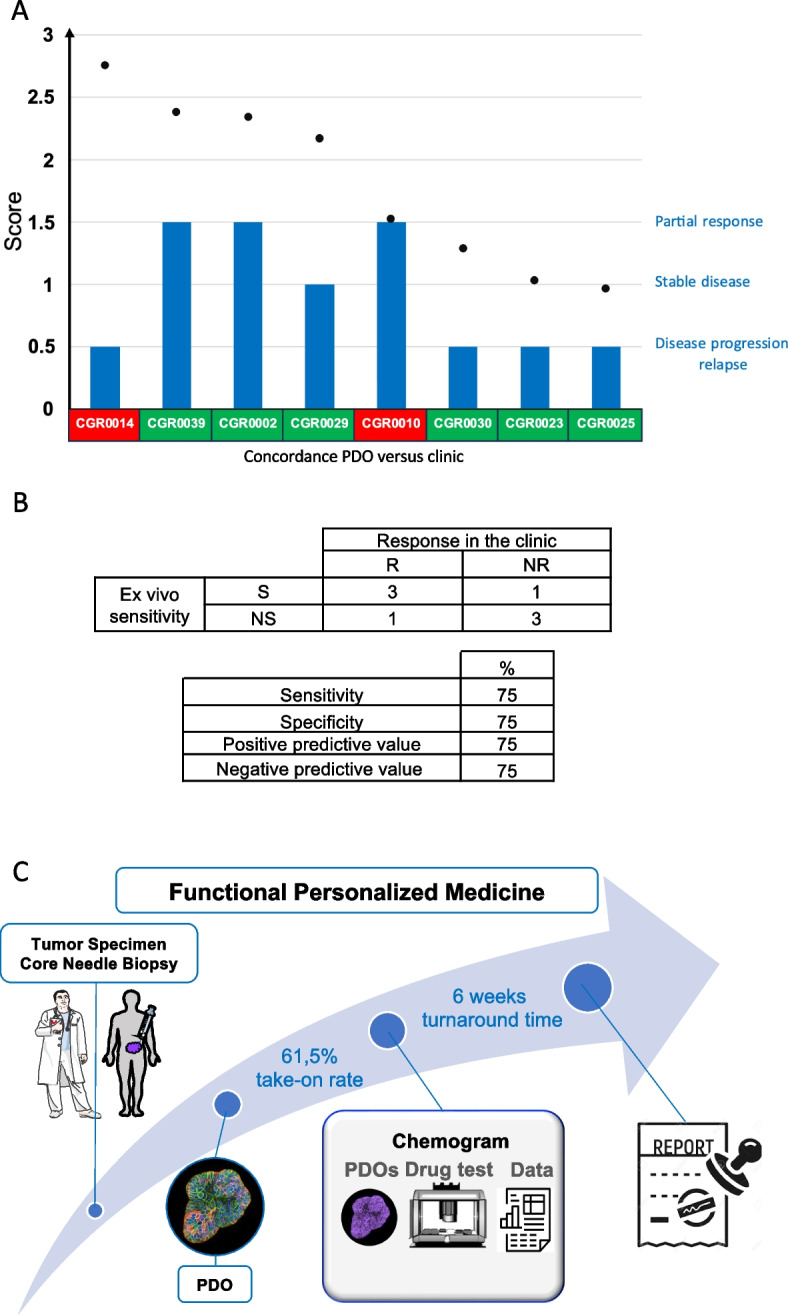
Results: A total of 25 PDOs were successfully established, harboring 94% concordance with the genomic profile of the tumor they were derived from. The take-on rate for PDOs derived from core needle biopsies was 61.5%. A chemogram was obtained with a 6-week median turnaround time (range, 4-10 weeks). At least one hit (mean 6.16) was identified for 92% of the PDOs. The number of hits was inversely correlated to disease metastatic dissemination and the number of lines of treatment the patient received. The chemograms were compared to clinical data obtained from 8 patients and proved to be predictive of their response with 75% sensitivity and specificity.
Conclusions: We show that PDO-based drug tests can be achieved in the frame of routine clinical practice. The chemogram could provide clinicians with a decision-making tool to tailor patient treatment. Thus, PDO-based functional precision oncology should now be tested in interventional trials assessing its clinical utility for patients who do not harbor activable genomic alterations or have developed resistance to standard of care treatments.
Keywords: Chemogram; Colorectal cancer; Organoids; Precision medicine.
© 2023. Italian National Cancer Institute ‘Regina Elena’.
Conflict of interest statement
F.J and J.C are co-founders of ORAKL Oncology. The authors declare that they have no competing interests.
Figures
References
-
- Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;S0923–7534(22):04192–4198. - PubMed
-
- Massard C, Michiels S, Ferté C, Le Deley MC, Lacroix L, Hollebecque A, et al. High-Throughput Genomics and Clinical Outcome in Hard-to-Treat Advanced Cancers: Results of the MOSCATO 01 Trial. Cancer Discov. 2017;7(6):586–595. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
