

Risk Factors and Mortality of Elderly Patients with Hospital-Acquired Pneumonia of Carbapenem-Resistant Klebsiella pneumoniae Infection
- PMID: 37881505
- PMCID: PMC10595997
- DOI: 10.2147/IDR.S431085
Risk Factors and Mortality of Elderly Patients with Hospital-Acquired Pneumonia of Carbapenem-Resistant Klebsiella pneumoniae Infection
Abstract
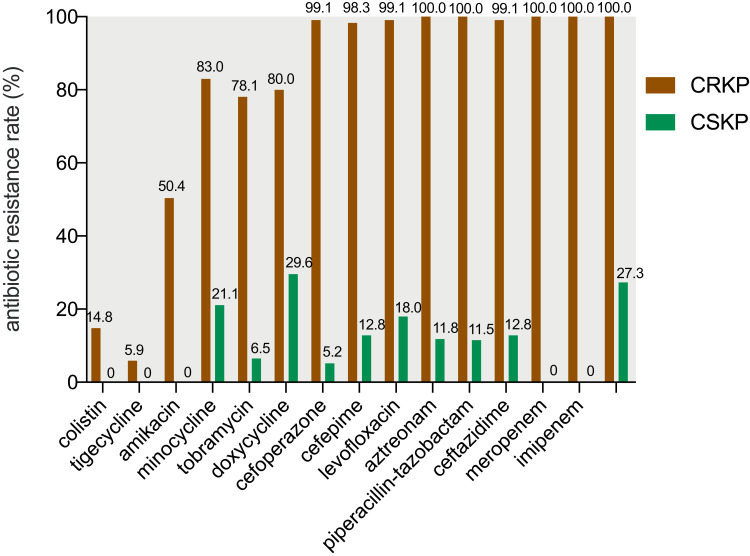
Purpose: Hospital-acquired pneumonia (HAP) caused by carbapenem-resistant K. pneumoniae (CRKP), especially in elderly patients, results in high morbidity and mortality. Studies on risk factors, mortality, and antimicrobial susceptibility of CRKP pulmonary infection among elderly patients are lacking.
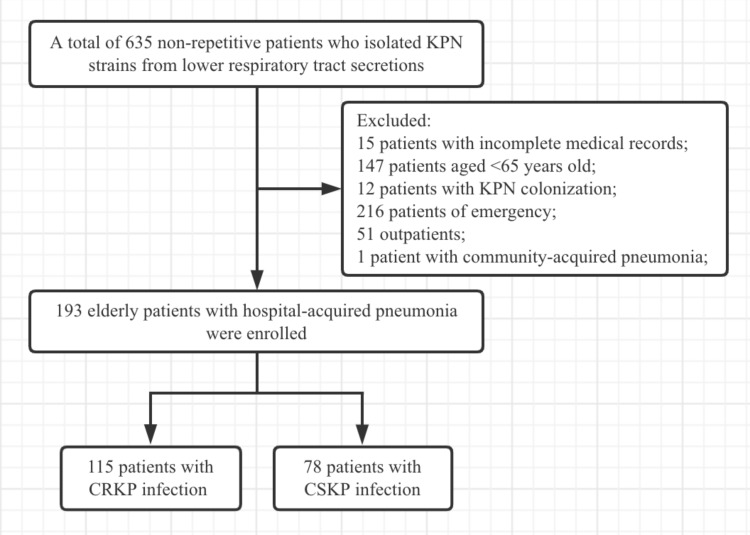
Patients and methods: A retrospective case-control study was conducted from January 2019 to December 2021. The elderly inpatients (≥65 years) who were diagnosed with HAP caused by K. pneumoniae were enrolled. Clinical data were collected. Univariate and multivariate logistic regression analyses were used to identify risk factors. Propensity score matching was used to minimize the effect of potential confounding variables. Kaplan-Meier analysis was used to compare survival.
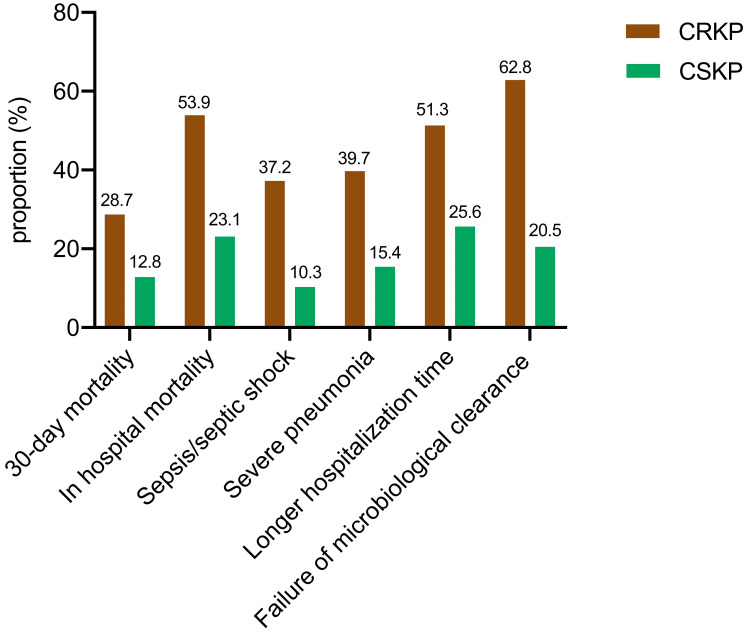
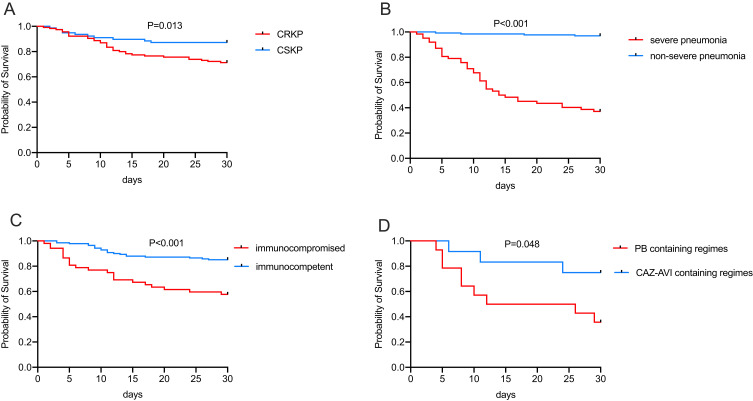
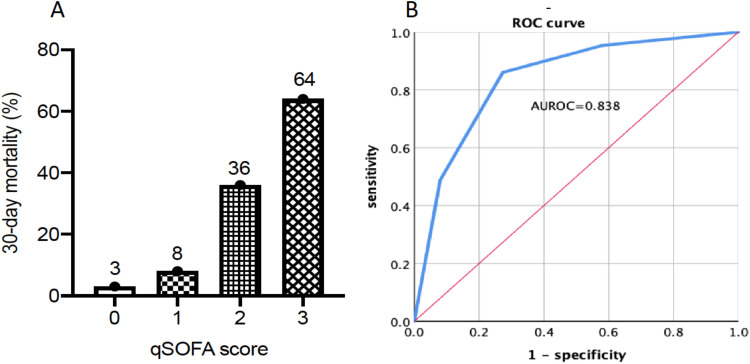
Results: A total of 115 patients with CRKP infection and 78 patients with carbapenem-susceptible K. pneumoniae (CSKP) infection were recruited. There were four independent risk factors for CRKP infection: history of intensive care unit (ICU) stays from hospital admission to positive respiratory specimen culture for K. pneumoniae (odds ratio (OR)=2.530), Charlson comorbidity index score ≥3 (OR = 2.420), prior exposure to carbapenems (OR = 5.280), and prior K. pneumoniae infection or colonization in the preceding 3 years (OR = 18.529). The all-cause 30-day mortality was 22.3%, the mortality of CRKP and CSKP infection was 28.7% and 12.8%, respectively. Independent risk factors for mortality included: older age (OR = 1.107), immunocompromised patients (OR = 8.632), severe pneumonia (OR = 51.244), quick Sepsis-related Organ Failure Assessment (qSOFA) score ≥2 (OR = 6.187), exposure to tigecycline before infection (OR = 24.702), and prolonged ICU stay (OR = 0.987). Thirty-day mortality was significantly lower in patients receiving ceftazidime-avibactam (CAZ-AVI) containing regimens than patients receiving polymyxin B sulfate (PB) containing regimens (P = 0.048). qSOFA score had a good prognostic effect [area under receiver operating characteristic curve (AUROC) of 0.838].
Conclusion: Active screening of CRKP for the high-risk populations, especially elderly patients, is significant for early detection and successful management of CRKP infection.
Keywords: CRKP; CSKP; ceftazidime-avibactam; elderly; hospital-acquired pneumonia; qSOFA.
© 2023 Zhou et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Healthcare-associated carbapenem-resistant Klebsiella pneumoniae bloodstream infections: Risk factors, mortality, and antimicrobial susceptibility, 2017-2019.J Formos Med Assoc. 2021 Nov;120(11):1994-2002. doi: 10.1016/j.jfma.2021.04.014. Epub 2021 May 5. J Formos Med Assoc. 2021. PMID: 33962811
-
[Klebsiella pneumoniae Infections in the Intensive Care Unit: Risk Factors Related to Carbapenem Resistance and Patient Mortality].Mikrobiyol Bul. 2020 Jul;54(3):378-391. doi: 10.5578/mb.69679. Mikrobiyol Bul. 2020. PMID: 32755515 Turkish.
-
The Colonization of Carbapenem-Resistant Klebsiella pneumoniae: Epidemiology, Resistance Mechanisms, and Risk Factors in Patients Admitted to Intensive Care Units in China.J Infect Dis. 2020 Mar 16;221(Suppl 2):S206-S214. doi: 10.1093/infdis/jiz622. J Infect Dis. 2020. PMID: 32176790
-
Relationship between antibiotic exposure and carbapenem-resistant Klebsiella pneumoniae infection within four types of control patients: A systematic review and meta-analysis.J Glob Antimicrob Resist. 2023 Jun;33:137-151. doi: 10.1016/j.jgar.2023.02.020. Epub 2023 Mar 10. J Glob Antimicrob Resist. 2023. PMID: 36906174
-
Risk factors for carbapenem-resistant Klebsiella pneumoniae infection relative to two types of control patients: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2020 Jan 31;9(1):23. doi: 10.1186/s13756-020-0686-0. Antimicrob Resist Infect Control. 2020. PMID: 32005246 Free PMC article.
Cited by
-
Comparative analysis of clinical characteristics and outcomes between carbapenem-resistant and carbapenem-sensitive Klebsiella pneumoniae infections: insights from a tertiary hospital in Northern China.Front Med (Lausanne). 2025 Feb 5;12:1499057. doi: 10.3389/fmed.2025.1499057. eCollection 2025. Front Med (Lausanne). 2025. PMID: 39975685 Free PMC article.
-
The prognostic value of neutrophil-to-lymphocyte ratio in adult carbapenem-resistant Klebsiella pneumoniae infection: a retrospective cohort study.Front Cell Infect Microbiol. 2024 Nov 28;14:1461325. doi: 10.3389/fcimb.2024.1461325. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39669277 Free PMC article.
-
Clinical and Microbiological Risk Factors for 30-Day Mortality of Bloodstream Infections Caused by OXA-48-Producing Klebsiella pneumoniae.Pathogens. 2023 Dec 21;13(1):11. doi: 10.3390/pathogens13010011. Pathogens. 2023. PMID: 38276157 Free PMC article.
-
Study on the predictive value of APACHE II score and neurogenic dysphagia in carbapenem-resistant Klebsiella pneumoniae.Medicine (Baltimore). 2024 Dec 13;103(50):e40858. doi: 10.1097/MD.0000000000040858. Medicine (Baltimore). 2024. PMID: 39686489 Free PMC article.
-
Emergence of Tigecycline-Nonsusceptible Carbapenem-Resistant Klebsiella pneumoniae with Metallo-β-Lactamase and Transferable Ceftazidime-Avibactam Resistance in China.Pathogens. 2025 Mar 4;14(3):253. doi: 10.3390/pathogens14030253. Pathogens. 2025. PMID: 40137738 Free PMC article.
References
-
- Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017:50. doi:10.1183/13993003.00582-2017 - DOI - PubMed
LinkOut - more resources
Full Text Sources
