

Selective dysfunction of the crural diaphragm in patients with chronic restrictive and obstructive lung disease
- PMID: 37882102
- PMCID: PMC10842479
- DOI: 10.1111/nmo.14699
Selective dysfunction of the crural diaphragm in patients with chronic restrictive and obstructive lung disease
Abstract
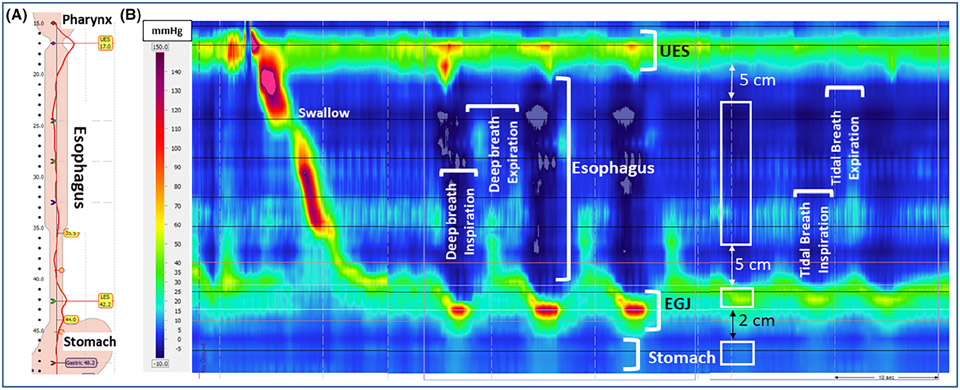
Background: Gastroesophageal reflux (GER) is known to be associated with chronic lung diseases. The driving force of GER is the transdiaphragmatic pressure (Pdi) generated mainly by costal and crural diaphragm contraction. The latter also enhances the esophagogastric junction (EGJ) pressure to guard against GER.
Methods: The relationship between Pdi and EGJ pressure was determined using high resolution esophageal manometry in patients with interstitial lung disease (ILD, n = 26), obstructive lung disease (OLD, n- = 24), and healthy subjects (n = 20).
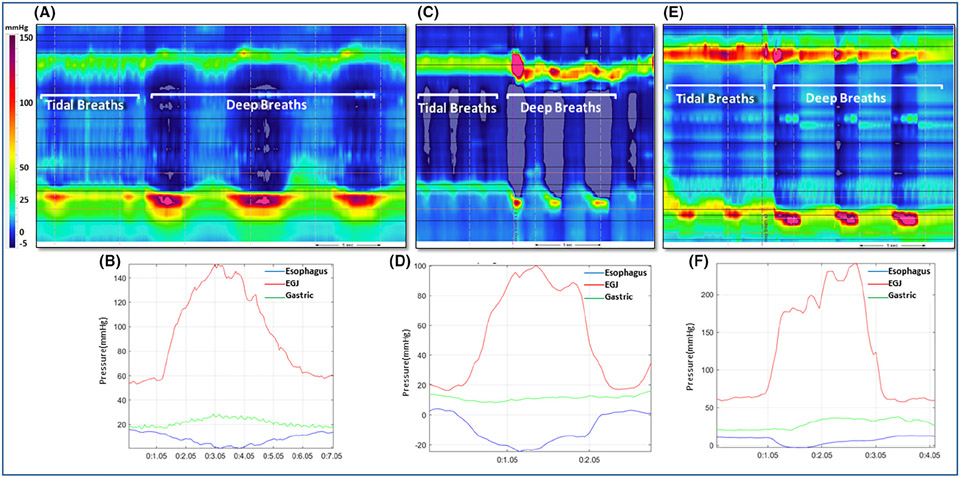
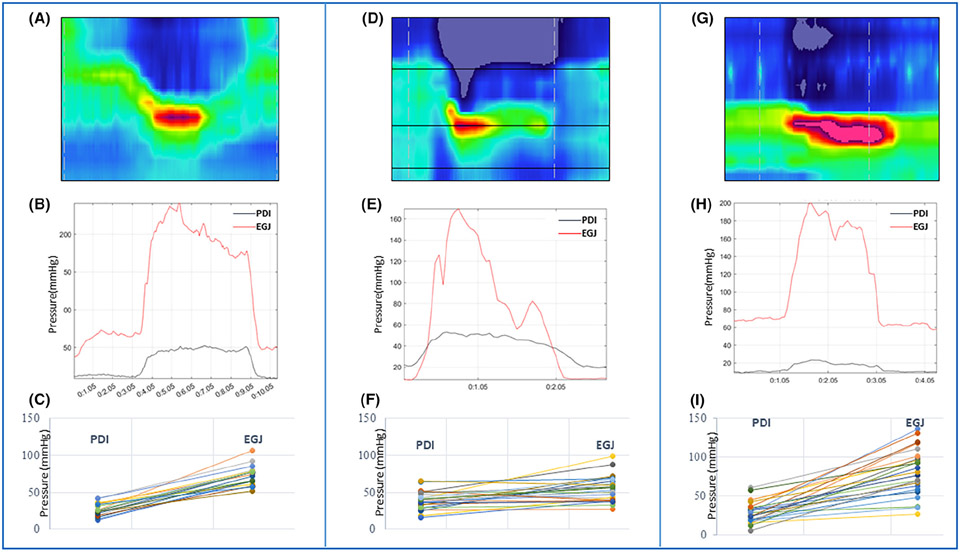
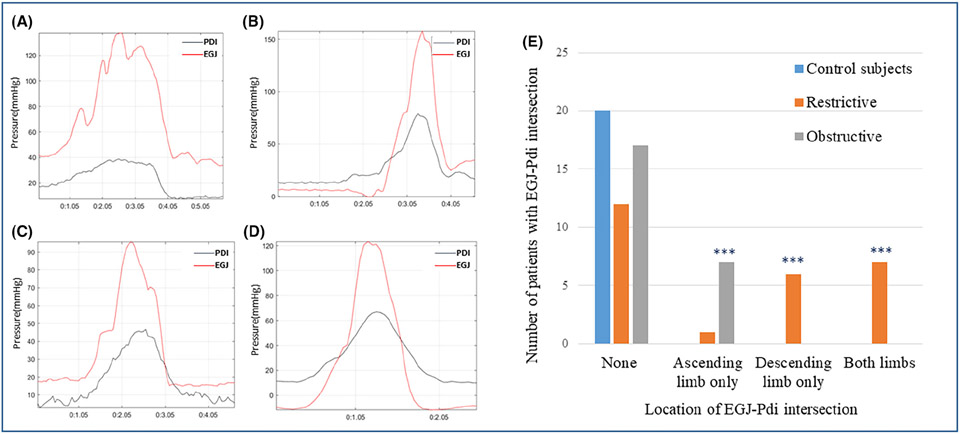
Key results: The patient groups did not differ with respect to age, gender, BMI, and pulmonary rehabilitation history. Patients with ILD had significantly higher Pdi but lower EGJ pressures as compared to controls and OLD patients (p < 0.001). In control subjects, the increase in EGJ pressure at all-time points during inspiration was greater than Pdi. In contrast, the EGJ pressure during inspiration was less than Pdi in 14 patients with ILD and 7 patients with OLD. The drop in EGJ pressure was usually seen after the peak Pdi in ILD group (p < 0.0001) and before the peak Pdi in OLD group, (p = 0.08). Nine patients in the ILD group had sliding hiatus hernia, compared to none in control subjects (p = 0.003) and two patients in the OLD, (p = 0.04).
Conclusions and inferences: A higher Pdi and low EGJ pressure, and dissociation between Pdi and EGJ pressure temporal relationship suggests selective dysfunction of the crural diaphragm in patients with chronic lung diseases and may explain the higher prevalence of GERD in ILD as seen in previous studies.
Keywords: crural diaphragm; esophagogastric junction; gastroesophageal reflux; hiatus hernia; lower esophageal sphincter; transdiaphragmatic pressure gradient.
© 2023 The Authors. Neurogastroenterology & Motility published by John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
The authors have no conflict of interest to declare.
Figures
Similar articles
-
Botox injection into the lower esophageal sphincter induces hiatal paralysis and gastroesophageal reflux.Am J Physiol Gastrointest Liver Physiol. 2020 Jan 1;318(1):G77-G83. doi: 10.1152/ajpgi.00238.2019. Epub 2019 Oct 7. Am J Physiol Gastrointest Liver Physiol. 2020. PMID: 31589467 Free PMC article.
-
Esophagogastric Junction Morphology and Distal Esophageal Acid Exposure.Dig Dis Sci. 2016 Dec;61(12):3537-3544. doi: 10.1007/s10620-016-4331-y. Epub 2016 Oct 11. Dig Dis Sci. 2016. PMID: 27730315
-
Correlation between novel 3D high-resolution manometry esophagogastric junction metrics and pH-metry in reflux disease patients.Neurogastroenterol Motil. 2018 Sep;30(9):e13344. doi: 10.1111/nmo.13344. Epub 2018 Apr 11. Neurogastroenterol Motil. 2018. PMID: 29644765
-
Current concepts of the antireflux barrier.Gastroenterol Clin North Am. 1990 Sep;19(3):501-16. Gastroenterol Clin North Am. 1990. PMID: 2228160 Review.
-
Evaluation of the esophagogastric junction using high resolution manometry and esophageal pressure topography.Neurogastroenterol Motil. 2012 Mar;24 Suppl 1:11-9. doi: 10.1111/j.1365-2982.2011.01829.x. Neurogastroenterol Motil. 2012. PMID: 22248103 Review.
Cited by
-
Determinants of cough-related quality of life in interstitial lung diseases.BMC Pulm Med. 2024 Aug 29;24(1):427. doi: 10.1186/s12890-024-03218-z. BMC Pulm Med. 2024. PMID: 39210302 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
