

Twice-Daily Dosing of Dolutegravir in Infants on Rifampicin Treatment: A Pharmacokinetic Substudy of the EMPIRICAL Trial
- PMID: 37882611
- PMCID: PMC10954323
- DOI: 10.1093/cid/ciad656
Twice-Daily Dosing of Dolutegravir in Infants on Rifampicin Treatment: A Pharmacokinetic Substudy of the EMPIRICAL Trial
Abstract
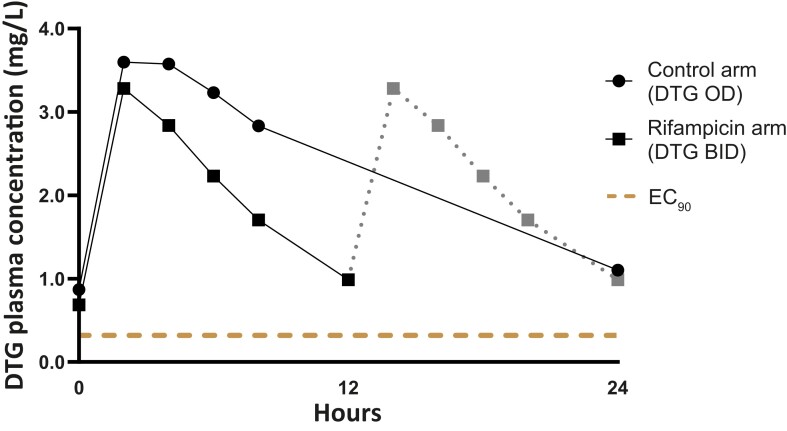
Background: We evaluated dolutegravir pharmacokinetics in infants with human immunodeficiency virus (HIV) receiving dolutegravir twice daily (BID) with rifampicin-based tuberculosis (TB) treatment compared with once daily (OD) without rifampicin.
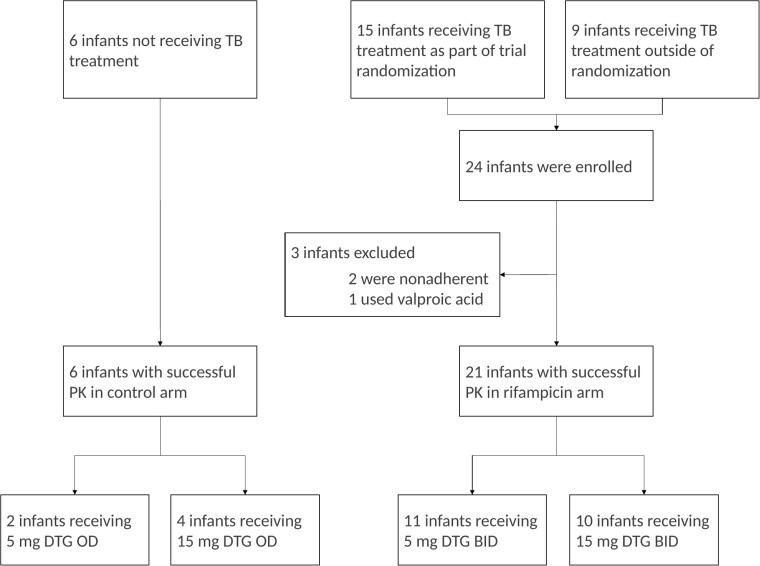
Methods: Infants with HIV aged 1-12 months, weighing ≥3 kg, and receiving dolutegravir BID with rifampicin or OD without rifampicin were eligible. Six blood samples were taken over 12 (BID) or 24 hours (OD). Dolutegravir pharmacokinetic parameters, HIV viral load (VL) data, and adverse events (AEs) were reported.
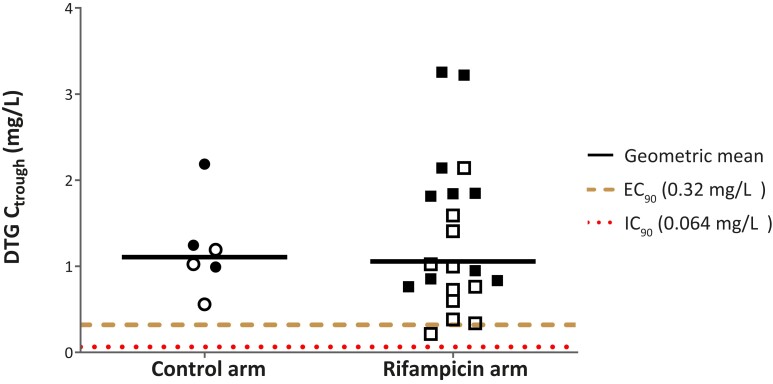
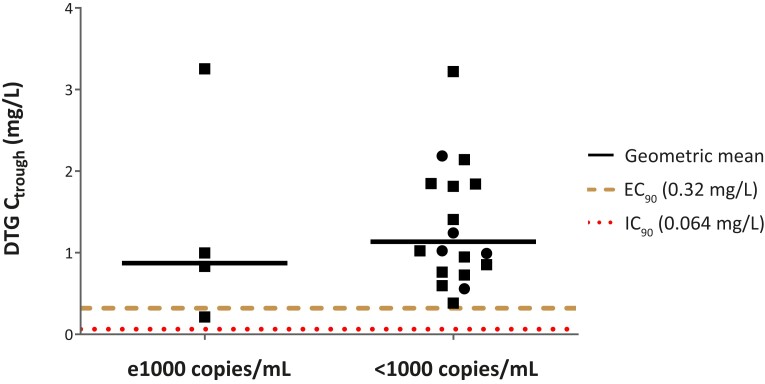
Results: Twenty-seven of 30 enrolled infants had evaluable pharmacokinetic curves. The median (interquartile range) age was 7.1 months (6.1-9.9), weight was 6.3 kg (5.6-7.2), 21 (78%) received rifampicin, and 11 (41%) were female. Geometric mean ratios comparing dolutegravir BID with rifampicin versus OD without rifampicin were area under curve (AUC)0-24h 0.91 (95% confidence interval, .59-1.42), Ctrough 0.95 (0.57-1.59), Cmax 0.87 (0.57-1.33). One infant (5%) receiving rifampicin versus none without rifampicin had dolutegravir Ctrough <0.32 mg/L, and none had Ctrough <0.064 mg/L. The dolutegravir metabolic ratio (dolutegravir-glucuronide AUC/dolutegravir AUC) was 2.3-fold higher in combination with rifampicin versus without rifampicin. Five of 82 reported AEs were possibly related to rifampicin or dolutegravir and resolved without treatment discontinuation. Upon TB treatment completion, HIV viral load was <1000 copies/mL in 76% and 100% of infants and undetectable in 35% and 20% of infants with and without rifampicin, respectively.
Conclusions: Dolutegravir BID in infants receiving rifampicin resulted in adequate dolutegravir exposure, supporting this treatment approach for infants with HIV-TB coinfection.
Keywords: HIV; dolutegravir; drug–drug interaction; infants; rifampicin.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. A. C. reports research grants from ViiV Healthcare, Gilead Sciences, and Merck, all paid to institution; consulting fees for serving on a Gilead advisory board and Merck advisory board, all paid to institution; participation in the Pharmacokinetics and Safety of DolutegravIr in Neonate (PETITE) study on a data and safety monitoring board (DSMB) and in the Doravirine Dose Optimisation in Pregnancy (DORADO) study on a DSMB; and a role as member of Paediatric Antiretroviral Working Group (PAWG) and as co-chair of the HIV, Hepatitis and STIs Pregnancy and Breastfeeding Therapeutics Working Group. P. R. reports grants from ViiV Healthcare and Merck. D. B. reports being cofounder of Global DDI solutions and that his employer, RadboudUMC, has received grants from ViiV Healthcare, Gilead Sciences, Merck, and Pfizer. W. C. B. reports support for attending the Pediatrics & HIV 2023 Conference in Brisbane, Australia, to present an EMPIRICAL abstract with study funding. V. M. reports support for attending international conference from Viatris and participation on a DSMB and advisory board for ViiV Healthcare. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization . Global tuberculosis report 2022. Geneva, Switzerland: World Health Organization, 2022.
